1. Introduction
The development of muscular strength and movement skills in youth is a key outcome for leading health authorities, long-term athletic development models, and physical education curricula [
1,
2,
3]. Reduction of chronic diseases, reduced injury risk, improved health and well-being, and longevity in physical activity are all products of improving muscular strength and movement skills in youth [
4,
5,
6,
7,
8,
9]. Previous research investigating the development of movement skills has focused mainly on fundamental movement skills in youth, which include locomotive, stabilisation, and manipulation skills [
6,
7,
10,
11,
12,
13,
14]. Lloyd et al. [
15] introduced the concept of athletic motor skill competencies (AMSC) to guide strength and conditioning coaches and physical education teachers in developing young people’s athleticism. The AMSC are considered foundational movement skills that underpin athletic movements, providing youth with the skills needed to safely and effectively participate in physical activity with confidence and competence [
15,
16]. The AMSC incorporate skills such as lower-body bilateral and unilateral movements, upper-body pushing and pulling, anti-rotation and core bracing, acceleration, deceleration and reacceleration, jumping, landing and rebounding mechanics, and traditional fundamental movements skills [
15,
17,
18]. To assess the AMSC, movement screening can be implemented, using process orientated measures to assess movement limitations and biomechanical deficits in individual movements against pre-determined performance criteria [
19].
The AMSC are vital to the habitual development of athleticism in youth, and central to long-term athletic development [
16]. Importantly, a recent editorial has highlighted the need for the AMSC to be considered a central aim in physical education [
20]. In the UK, the four key aims of physical education are to develop competence to excel in a broad range of physical activities, get children active for sustained periods of time, engage in competitive sports, and lead healthy, active lives [
21]. Despite these aims, children in the UK currently do not meet recommended daily physical activity guidelines [
22], and participation in a game/sports curriculum does not ensure the development of muscular strength, physical fitness, or AMSC [
15]. Globally, only a small proportion (20%) of adolescents are hitting daily recommended physical activity guidelines [
22]. The World Health Organization has identified national success stories in the quest of promoting physical activity through the education sector or in schools [
23]. For example, in Denmark, 45 min of daily physical activity was introduced in 2013. Finland introduced the “Finnish schools on the move” initiative, which was piloted in 2010–2012 with schools implementing their own plans to increase physical activity during lessons, school breaks, and after school. The UK was recognised for the daily mile initiative, which was launched in 2017 and aimed to encourage children to run or jog for at least 15 min every day.
One key determining factor for health outcomes and levels of physical activity in children is the concept of physical literacy, which is underpinned by motor competence, motivation, and confidence [
24,
25]. Previous research in physical literacy has identified that two current paradigms exist [
25]. The first paradigm, based on research by Whitehead, considers physical literacy as a holistic ability, with individuals being able to skilfully interact with their ever changing environments with motivation, confidence, and physical competence [
26,
27]. The second paradigm, the long-term athletic development approach, focuses solely on the physical components of physical literacy [
28]. However, the paradigms should not be considered mutually exclusive. In this study we consider physical literacy to be fluid and flexible with no definitive boarders, somewhat ambiguous, akin to the pluralist view of concepts as in the recent Young et al. [
29] paper. Thus, there is a need to consider relationships between AMSC and psychological constructs.
Little is known about the associations between AMSC and psychological constructs in school children and if interactions differ between the sexes. In a population of Australian adolescent school children (14 ± 0.5 years), movement screen scores demonstrated significant correlations to resistance training self-efficacy and motivation to exercise [
30]. In younger children (6–7 years), 10 weeks of strength and conditioning focusing on the development of movement resulted in significant improvements in physical self-efficacy in boys but not girls [
31]. However, it is still unknown whether children possessing higher levels of AMSC and psychological constructs differ from those scoring lower in AMSC movement screens and if variations between the sexes exist. To understand the importance of the AMSC in the holistic development of youth, the interaction between affective themes such as confidence, motivation, and perceptions of physical competence merit investigation [
25]. Intrinsic motivation is related to affective change during both moderate and hard intensity exercise in adolescents and plays an important role in motor performance and learning [
32,
33]. Physical self-efficacy (an individual’s situational beliefs in their own abilities [
34]) is a significant precursor to physical activity with mediating effects on motivation [
35]. Investigations into school children need to consider boys and girls separately, as factors such as maturation timing, physical growth, and psychological constructs vary between the sexes [
36,
37,
38]. Differences in the rate and timing of growth between the sexes become most prominent with the onset of the pubertal growth spurt, with large divergences between boys and girls impacting physical performance [
39,
40].
Previous research has identified associations between AMSC and muscular strength in school children, however such studies have been exclusive to same sex comparisons [
41,
42]. To the authors’ knowledge, only one study has previously investigated the relationship between AMSC, muscular fitness, and psychological constructs [
30]. The authors focused on the prevalence and correlates of AMSC in school children, revealing significant associations between muscular fitness and AMSC (males: β = 0.31,
p ≤ 0.001; females β = 0.33,
p ≤ 0.001), but AMSC associations to autonomous motivation were only small in magnitude (β ≤ 0.2). However, it is still unknown whether higher levels of AMSC demonstrate associations to BMI, physical performance, and psychological constructs. It is hypothesised that the AMSC may have relationships with physical performance and psychological constructs with variations between the sexes. Therefore, the aims of this study were to (1) examine the relationships between maturity and AMSC, BMI, physical performance and psychological constructs, and (2) identify differences between boys and girls and higher and lower levels of AMSC.
4. Discussion
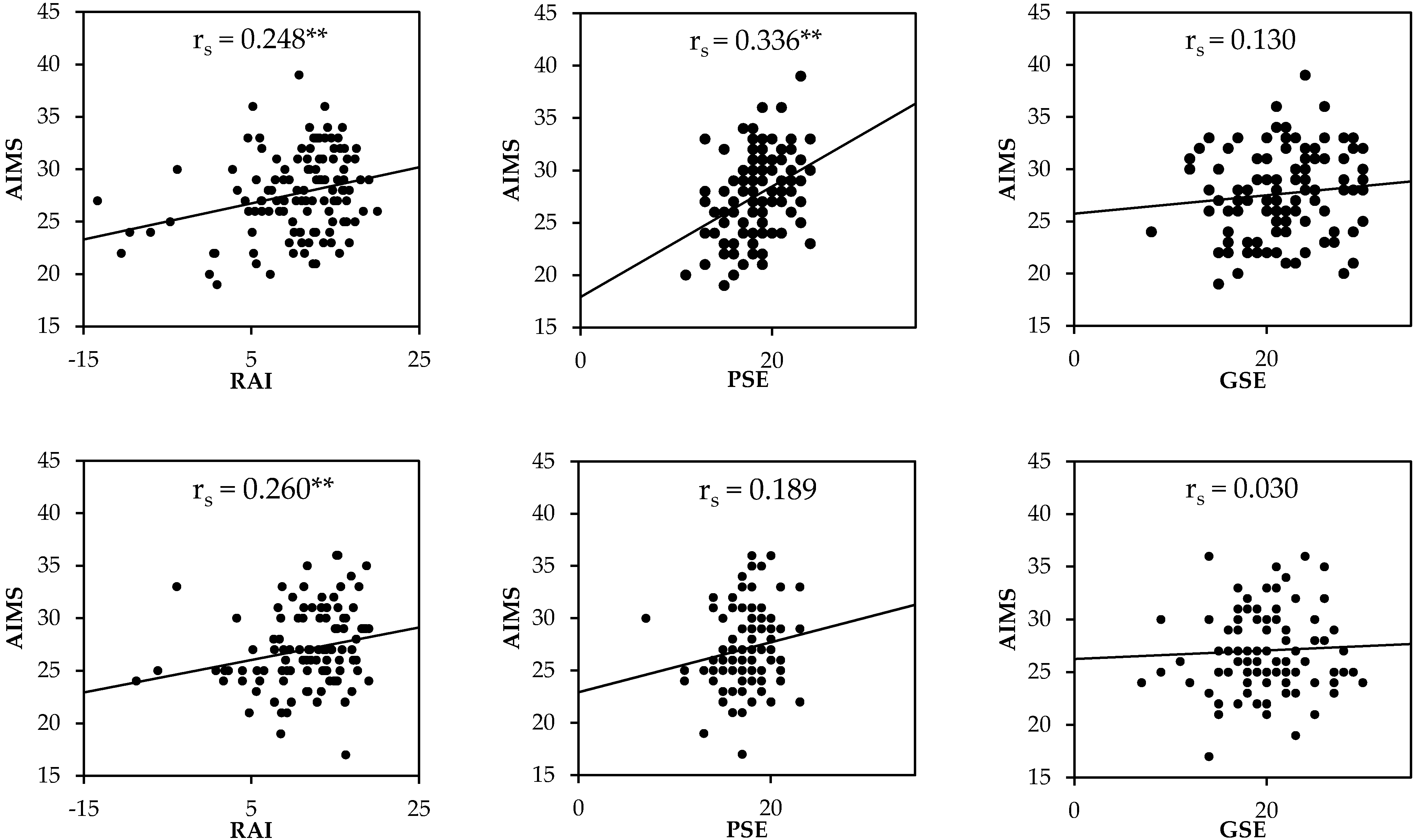
This study examined the relationship between AMSC movement screen scores, sex, maturity offset, BMI, physical performance, and selected psychological constructs in boys and girls. The findings indicate that the ability to perform AMSC in the AIMS are positively and significantly correlated to physical performance, motivation to exercise, and physical self-efficacy in both male and female children. However, it should also be recognized that where significant relationships were observed, they were small to moderate in strength. When grouped according to the composite AIMS score, higher competency boys and girls jumped significantly further, were more motivated to exercise, and possessed greater physical self-efficacy than those with lower AIMS scores. Cumulatively, the findings indicate some important association between AMSC movement screen scores, physical performance, and psychological constructs in boys and girls.
4.1. Relationships
Maturity offset demonstrated moderate associations with BMI in both males and females, which may be attributed to maturation as it is a time that sees major changes and variation between the sexes in growth and stature [
37,
39,
61]. The only other relationship to maturity offset was a small correlation with standing long jump performance in females. Although only a small relationship in the present study, girls have been shown to experience a decrease in neuromuscular control over the course of maturation [
62]. Previous research has demonstrated a maturation effect between movement competency assessments and jump performance measures [
63,
64]. Yet, such studies often sample participants with a large range in age and maturity, thereby increasing sample heterogeneity and potentially inflating the correlations [
63,
64]. Multiple internal factors can influence the development of AMSC, including growth, maturation, adolescent awkwardness, and neural development [
62,
65,
66,
67]. Nevertheless, the weak relationships between maturity status and AMSC may reflect the differential timings of the development of the central nervous system and movement competence [
12,
68,
69]. It may then be that AMSC fail to naturally develop further in early adolescence unless the environment a child is exposed to provides an adequate stimulus. This reinforces the importance of well-designed physical education curricula to promote the continued development of AMSC as boys and girls move into secondary school.
Associations between maturity status and BMI were present in both sexes, which may be attributed to the population being circa puberty, a period characterized by marked somatic changes [
39,
65,
70]. There were small to moderate relationships between BMI, physical performance, and psychological constructs in boys and girls. Boys demonstrated stronger associations between BMI and AMSC-based assessments (AIMS and TJA), whereas BMI in girls was more strongly correlated to psychological constructs. The impact of BMI on adolescents’ self-perceptions is strongly influenced by their wider sociocultural context, which has previously been shown to influence girls more strongly than boys. [
71] Furthermore, the female group was characterized by lower levels of physical self-efficacy and self-esteem in this study, which reflects previous findings that the greatest decline in body satisfaction in adolescents is experienced by females [
72]. Longitudinal evidence has supported a negative association between weight status and movement competency [
73,
74]. In addition, an AMSC intervention conducted by Smith et al. [
75] was successful in positively mediating body composition and muscular fitness. Despite the difference in BMI between higher and lower AMSC groups nearing significance (
p < 0.06), the amount of shared variance between AMSC and BMI was relatively low (<20%), and thus associations should be interpreted with caution.
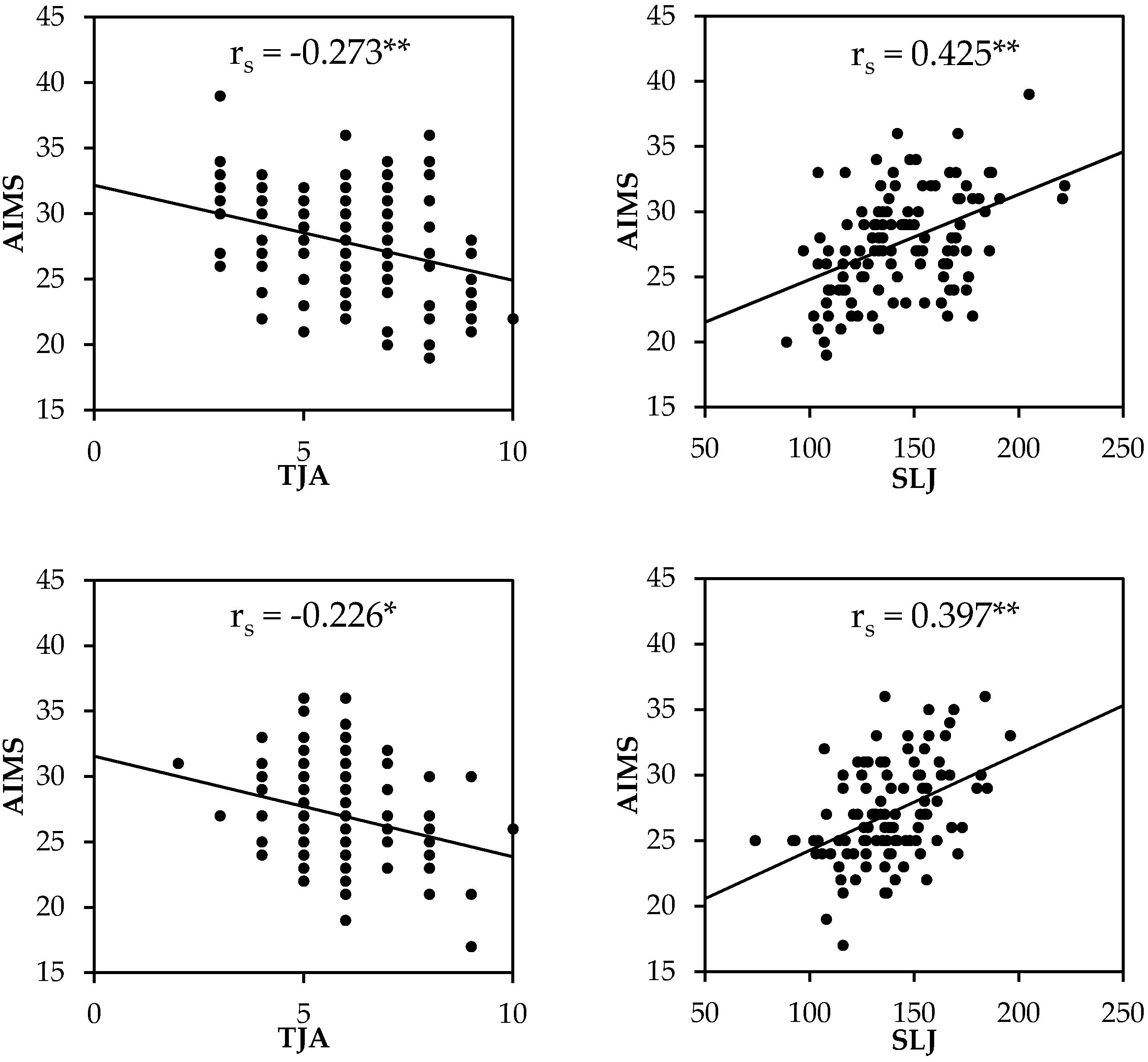
The standing long jump assessment demonstrated the strongest associations with the AIMS in both boys (
r = 0.425) and girls (
r = 0.397). The standing long jump is an assessment of lower limb strength and requires individuals to rapidly produce force in the lower limbs while maintaining postural control. Many of the movements in the AIMS, namely the overhead squat, lunge, and the brace with shoulder touch require activation and control of the musculature surrounding the trunk, hip, knee, and ankle [
76,
77]. Therefore, the standing long jump and AIMS are likely underpinned by the same neuromuscular control mechanisms and physical qualities, which might explain the significant moderate correlations reported. Associations between the AIMS and TJA were not as strong in comparison to the standing long jump. Although the TJA uses similar muscle groups as movements identified in the AIMS, it requires repeated maximal efforts with higher magnitudes and rates of force development [
78]. The repeated rapid maximal efforts with fatiguing elements to the TJA may explain the weaker associations to AIMS compared with the standing long jump.
4.2. Sex Differences
Boys and girls performed similarly across most AMSC measures, with competency in the push up the only difference between the sexes. This may be due to males out performing females in health-related fitness measures [
79]. There were more consistent differences in psychological constructs, with boys having significantly greater physical self-efficacy and global self-esteem. The study population scored below the normative average in physical performance respective to age with males scoring in the 30th percentile and females in the 40th percentile for the SLJ [
79]. Additionally, the population in this study scored below previous standards for AMSC (median AIMS score = 27–28) when compared with more athletic populations (mean AIMS score = 36) [
45]. The findings in this study align with previous research which has demonstrated that AMSC are not well developed in children [
30]. However, previous research has not considered the influence of AMSC on important psychological constructs linked to physical literacy. Additionally, previous research has not implemented movement screens as comprehensive as the AIMS at measuring movement consistency in the AMSC in youth [
19]. To that end, previous research implementing certain screening protocols may need reconsideration.
4.3. Differences between High and Low AIMS Score
When boys and girls were categorized by AIMS score, relationships between higher and lower competency groups and psychological constructs were the same in both sexes. Higher AIMS scores equated to significantly higher physical performance, jumping landing and rebounding mechanics, motivation to exercise, and physical self-efficacy in both sexes. School children possessing higher AIMS scores were 5.3% and 5.6% more motivated to exercise, performed 11.5% and 12.2% better physically, and had 6.6% and 8.3% lower body mass in males and females, respectively. There were no significant associations between AIMS and global self-esteem in both males and females or the high- or low-competency groups. Global self-esteem shows substantial stability over time with increasing stability from childhood to adolescence in both sexes; consequently, changes in physical competence may not be enough to impact self-esteem alone at global level [
80]. The current study builds on the absence of knowledge; establishing children’s physical performance differentiates AMSC ability with potential mediating effects on physical self-efficacy and motivation to exercise in school children.
4.4. Strengths
This study is the first of its kind to identify associations between AMSC and constructs from psychological domains in both boys and girls in a UK secondary school setting. The identified associations between the AMSC movement screen scores, motivation to exercise, and physical self-efficacy establish AMSC associations with affective themes within physical literacy [
25]. Thus, the study’s findings present the potential importance of developing young people’s AMSC to aid in positive psychological development. This study also provides novel between-sex comparisons, providing strength and conditioning practitioners normative values in AMSC in school children which may benchmark future research and coaching. Furthermore, this study furthers the field’s knowledge regarding the difference in psychological constructs of children who possess higher or lower abilities to perform the AMSC.
4.5. Limitations
This study only sampled children from schools in areas of lower socio-economic status, a known factor influencing motor performance [
81]. This study establishes relationships to AMSC, yet it is still unknown whether relationships between AMSC, sex, maturity, physical performance, and psychological constructs vary dependent on the socio-economic status of youth. Youth in areas of higher socioeconomic status may demonstrate higher levels of competency, as the population in this study scored below the 50th centile in physical performance [
79]. In addition, this study sampled children aged 11–13 years old, however the development of AMSC could be established earlier as a potential intervention to counteract the drop in physical activity levels, which begin as young as 7 years old [
82]. Thus, investigating AMSC in a more heterogeneous population with wide age ranges including childhood to late adolescence with a variety of socio-economic and cultural backgrounds could support knowledge surrounding the AMSC and their importance to youth. Intra-rater reliability of certain movements in the screen were moderate and some of the segmental analyses showed only slight agreement, which combined underlines the importance of determining an individual’s reliability at subjectively scoring movements. However, this study used protocols and measures that have shown to be valid and reliable in paediatric cohorts, and, in addition to the robust research design, this study contributes novel and rigorous findings to the paediatric literature.
4.6. Practical Recommendations
Body mass index has more of a mediating effect on AMSC then maturity status, therefore, interventions aiming to positively effect BMI may also enhance AMSC and other associated outcomes. Improving AMSC may have some associated benefits on increasing physical performance, physical self-efficacy, and motivation to exercise. However, it should be noted that as relationships were often only small to moderate it may also be necessary to develop each quality independently. Nevertheless, practitioners and teachers delivering physical activity interventions may consider strength training focusing on the development of AMSC to develop the psychological attributes of youth. Considering Young’s and Whitehead’s physical literacy connotations, the relationships between physical competence and affective psychological domains demonstrate the potential efficacy of enhancing AMSC to holistically develop physical literacy.






{kind=link}
{kind=link}