Pre-Exercise Blood Glucose Levels Determine the Amount of Orally Administered Carbohydrates during Physical Exercise in Individuals with Type 1 Diabetes—A Randomized Cross-Over Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Peak Cardio-Pulmonary Exercise (CPX) Testing
2.3. Diabetes Specificities
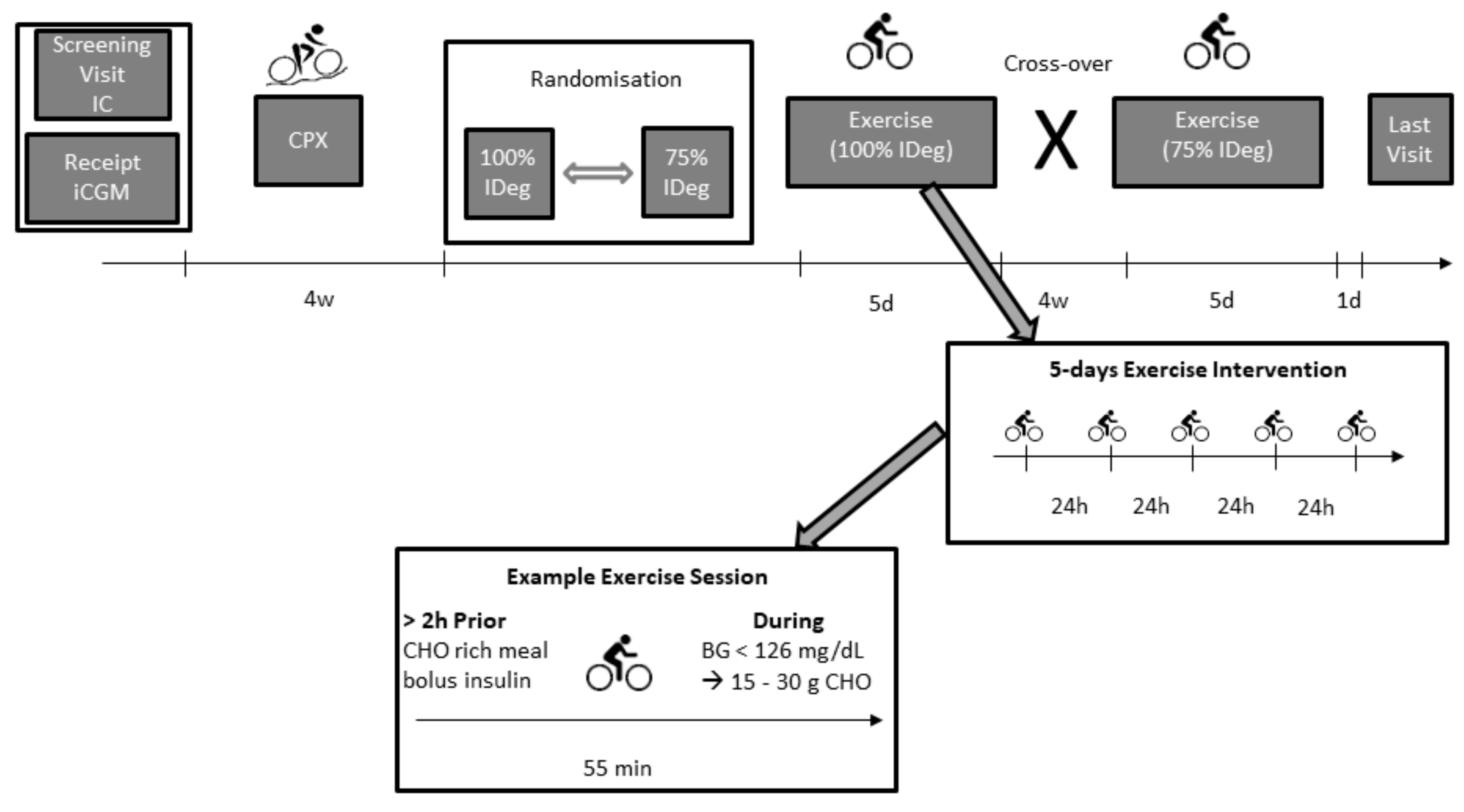
2.4. Moderate-Intensity Physical Exercise Periods
2.5. Statistical Analyses
3. Results
3.1. Participant Characteristics and Performance Data
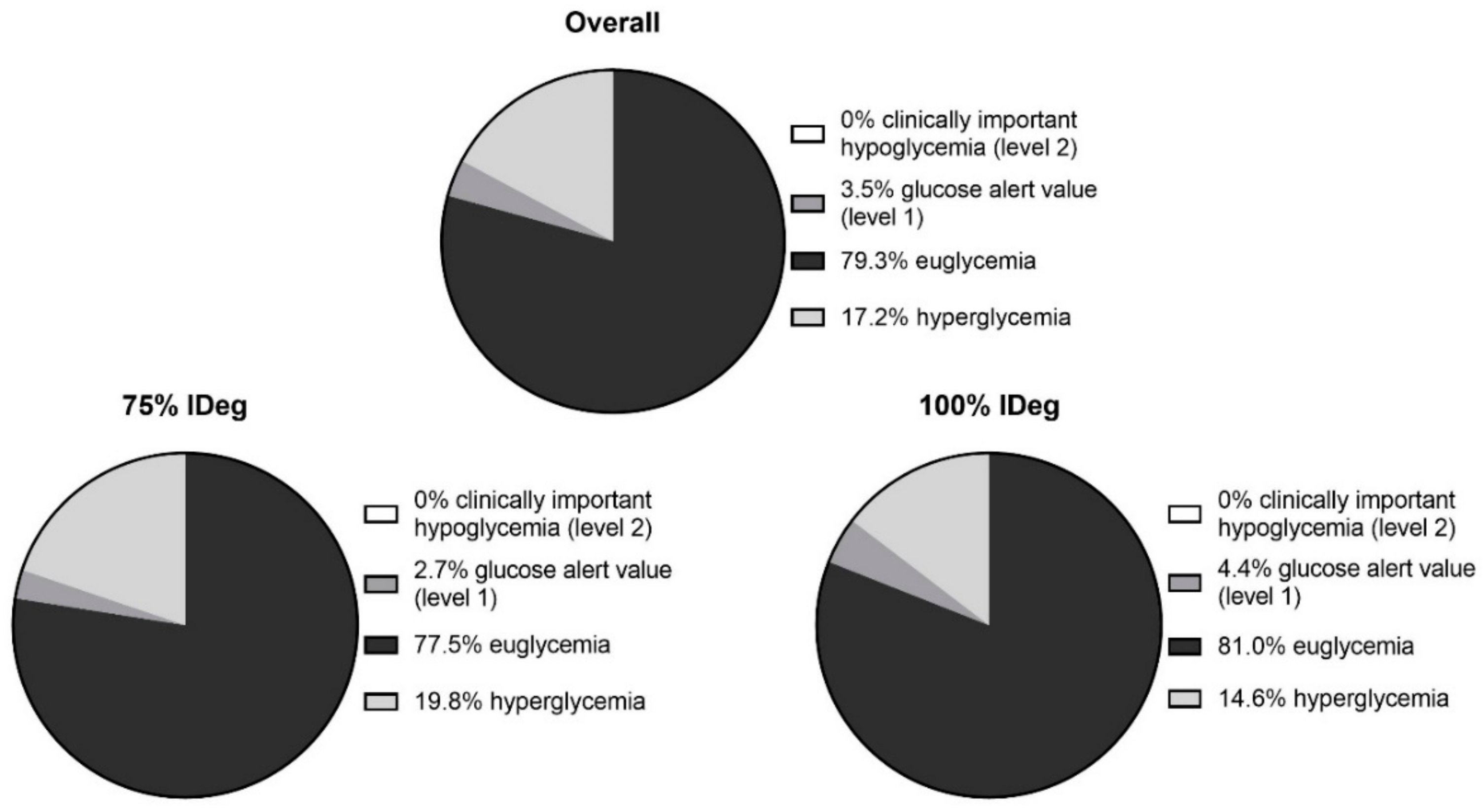
3.2. Diabetes-Specific Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical activity/exercise and diabetes: A position statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed]
- Chimen, M.; Kennedy, A.; Nirantharakumar, K.; Pang, T.T.; Andrews, R.; Narendran, P. What are the health benefits of physical activity in type 1 diabetes mellitus? A literature review. Diabetologia 2012, 55, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Salem, M.A.; Aboelasrar, M.A.; Elbarbary, N.S.; Elhilaly, R.A.; Refaat, Y.M. Is exercise a therapeutic tool for improvement of cardiovascular risk factors in adolescents with type 1 diabetes mellitus? A randomised controlled trial. Diabetol. Metab. Syndr. 2010, 2, 47. [Google Scholar] [CrossRef] [PubMed]
- Tikkanen-Dolenc, H.; Wadén, J.; Forsblom, C.; Harjutsalo, V.; Thorn, L.M.; Saraheimo, M.; Elonen, N.; Tikkanen, H.O.; Groop, P.-H.; FinnDiane Study Group. Physical Activity Reduces Risk of Premature Mortality in Patients With Type 1 Diabetes With and Without Kidney Disease. Diabetes Care 2017, 40, 1727–1732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brazeau, A.-S.; Rabasa-Lhoret, R.; Strychar, I.; Mircescu, H. Barriers to Physical Activity Among Patients With Type 1 Diabetes. Diabetes Care 2008, 31, 2108–2109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabasa-Lhoret, R.; Bourque, J.; Ducros, F.; Chiasson, J.L. Guidelines for premeal insulin dose reduction for postprandial exercise of different intensities and durations in type 1 diabetic subjects treated intensively with a basal-bolus insulin regimen (ultralente-lispro). Diabetes Care 2001, 24, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Moser, O.; Tschakert, G.; Mueller, A.; Groeschl, W.; Pieber, T.R.; Obermayer-Pietsch, B.; Koehler, G.; Hofmann, P. Effects of high-intensity interval exercise versus moderate continuous exercise on glucose homeostasis and hormone response in patients with type 1 diabetes mellitus using novel ultra-long-acting insulin. PLoS ONE 2015, 10, e0136489. [Google Scholar] [CrossRef]
- Riddell, M.C.; Gallen, I.W.; Smart, C.E.; Taplin, C.E.; Adolfsson, P.; Lumb, A.N.; Kowalski, A.; Rabasa-Lhoret, R.; McCrimmon, R.J.; Hume, C.; et al. Exercise management in type 1 diabetes: A consensus statement. Lancet Diabetes Endocrinol. 2017, 5, 377–390. [Google Scholar] [CrossRef]
- Rickels, M.; Dubose, S.; Wolpert, H.; Toschi, E.; Beck, R.; Cummins, M.; Newswanger, B.; Riddell, M. Mini-dose Glucagon as a Novel Approach to Prevent Exercise-Induced Hypoglycemia in Type 1 Diabetes. Diabetes Care 2017, 66, LB17. [Google Scholar] [CrossRef]
- Bussau, V.A.; Ferreira, L.D.; Jones, T.W.; Fournier, P.A. The 10-s maximal sprint: A novel approach to counter an exercise-mediated fall in glycemia in individuals with type 1 diabetes. Diabetes Care 2006, 29, 601–606. [Google Scholar] [CrossRef]
- Moser, O.; Tschakert, G.; Mueller, A.; Groeschl, W.; Hofmann, P.; Pieber, T.; Lawrence, J.; Koehler, G. Short-acting insulin reduction strategies for continuous cycle ergometer exercises in patients with type 1 diabetes mellitus. Asian J. Sports Med. 2017, 8, 42160. [Google Scholar] [CrossRef]
- Campbell, M.D.; Walker, M.; Trenell, M.I.; Luzio, S.; Dunseath, G.; Tuner, D.; Bracken, R.M.; Bain, S.C.; Russell, M.; Stevenson, E.J.; et al. Metabolic implications when employing heavy pre- and post-exercise rapid-acting insulin reductions to prevent hypoglycaemia in type 1 diabetes patients: A randomised clinical trial. PLoS ONE 2014, 9, e0097143. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, A.; Nirantharakumar, K.; Chimen, M.; Pang, T.T.; Hemming, K.; Andrews, R.C.; Narendran, P. Does Exercise Improve Glycaemic Control in Type 1 Diabetes? A Systematic Review and Meta-Analysis. PLoS ONE 2013, 8, e0058861. [Google Scholar] [CrossRef] [PubMed]
- Moser, O.; Eckstein, M.L.; McCarthy, O.; Deere, R.; Bain, S.C.; Haahr, H.L.; Zijlstra, E.; Bracken, R.M. Poor glycaemic control is associated with reduced exercise performance and oxygen economy during cardio-pulmonary exercise testing in people with type 1 diabetes. Diabetol. Metab. Syndr. 2017, 9, 93. [Google Scholar] [CrossRef] [PubMed]
- Moser, O.; Eckstein, M.L.; McCarthy, O.; Deere, R.; Bain, S.C.; Haahr, H.L.; Zijlstra, E.; Heise, T.; Bracken, R.M. Heart rate dynamics during cardio-pulmonary exercise testing are associated with glycemic control in individuals with type 1 diabetes. PLoS ONE 2018, 13, e0194750. [Google Scholar] [CrossRef] [PubMed]
- Riddell, M.C.; Zaharieva, D.P.; Tansey, M.; Tsalikian, E.; Admon, G.; Li, Z.; Kollman, C.; Beck, R.W. Individual glucose responses to prolonged moderate intensity aerobic exercise in adolescents with type 1 diabetes: The higher they start, the harder they fall. Pediatr. Diabetes 2018, 20, 99–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Randomization service for multicenter clinical trials. Available online: https://www.randomizer.at (accessed on 7 March 2019).
- Moser, O.; Eckstein, M.L.; Mueller, A.; Birnbaumer, P.; Aberer, F.; Koehler, G.; Sourij, C.; Kojzar, H.; Holler, P.; Simi, H.; et al. Reduction in insulin degludec dosing for multiple exercise sessions improves time spent in euglycaemia in people with type 1 diabetes: A randomised cross-over trial. Diabetes Obes. Metab. 2018, 21, 349–356. [Google Scholar] [CrossRef]
- Hofmann, P.; Tschakert, G. Special Needs to Prescribe Exercise Intensity for Scientific Studies. Cardiol. Res. Pract. 2011. [Google Scholar] [CrossRef]
- Study, I.H. Glucose Concentrations of Less Than 3.0 mmol/L (54 mg/dL) Should Be Reported in Clinical Trials: A Joint Position Statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2016, 40, 155–157. [Google Scholar] [CrossRef] [Green Version]
- Gallen, I.W.; Hume, C.; Lumb, A. Fuelling the athlete with type 1 diabetes. Diabetes Obes. Metab. 2011, 13, 130–136. [Google Scholar] [CrossRef] [PubMed]
- MØLLER, N.; JØRGENSEN, J.O.L.; ALBERTI, K.G.M.M.; FLYVBJERG, A.; SCHMITZ, O. Short-Term Effects of Growth Hormone on Fuel Oxidation and Regional Substrate Metabolism in Normal Man. J. Clin. Endocrinol. Metab. 1990, 70, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Galassetti, P.; Riddell, M.C. Exercise and type 1 diabetes (T1DM). Compr. Physiol. 2013, 3, 1309–1336. [Google Scholar] [CrossRef] [PubMed]
- West, D.J.; Stephens, J.W.; Bain, S.C.; Kilduff, L.P.; Luzio, S.; Still, R.; Bracken, R.M. A combined insulin reduction and carbohydrate feeding strategy 30 min before running best preserves blood glucose concentration after exercise through improved fuel oxidation in type 1 diabetes mellitus. J. Sports Sci. 2011, 29, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Moser, O.; Mader, J.; Tschakert, G.; Mueller, A.; Groeschl, W.; Pieber, T.; Koehler, G.; Messerschmidt, J.; Hofmann, P. Accuracy of Continuous Glucose Monitoring (CGM) during Continuous and High-Intensity Interval Exercise in Patients with Type 1 Diabetes Mellitus. Nutrients 2016, 8, 489. [Google Scholar] [CrossRef] [PubMed]
- Moser, O.; Yardley, J.; Bracken, R. Interstitial Glucose and Physical Exercise in Type 1 Diabetes: Integrative Physiology, Technology, and the Gap In-Between. Nutrients 2018, 10, 93. [Google Scholar] [CrossRef]
- Moser, O.; Eckstein, M.L.; Mueller, A.; Birnbaumer, P.; Aberer, F.; Koehler, G.; Sourij, C.; Kojzar, H.; Holler, P.; Simi, H.; et al. The impact of physical exercise on sensor performance of the Abbott Freestyle® Libre intermittently-viewed continuous glucose monitoring (iCGM) system in people with type 1 diabetes—A randomised cross-over trial. Diabet. Med. 2019. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Mean ± SD | Min–Max |
|---|---|---|
| Ppeak (Watt/kg) | 3.06 ± 0.89 | 1.57–4.34 |
| PLTP1 (Watt/kg) | 0.78 ± 0.31 | 0.25–1.40 |
| PLTP2 (Watt/kg) | 1.97 ± 0.56 | 0.98–2.73 |
| VO2peak (mL/kg/min) | 39 ± 12 | 22–64 |
| VO2LTP1 (mL/kg/min) | 16 ± 6 | 9–28 |
| VO2LTP2 (mL/kg/min) | 29 ± 10 | 14–46 |
| VEpeak (L/min) | 112 ± 36 | 75–173 |
| O2 pulsepeak (100 mL/b/kg) | 20.6 ± 5.7 | 13.9–34.0 |
| Variable | 75% IDeg | 100% IDeg | p-Value |
|---|---|---|---|
| VO2 of VO2peak % | 64 ± 7 | 62 ± 6 | 0.14 |
| HR of HRpeak % | 74 ± 6 | 73 ± 7 | 0.11 |
| VE of VEpeak % | 43 ± 8 | 43 ± 8 | 0.91 |
| RER of RERpeakx % | 75 ± 4 | 78 ± 2 | 0.09 |
| Lactate of Lactatepeak % | 20 ± 9 | 19 ± 7 | 0.57 |
| O2 pulse of O2pulsepeak % | 61 ± 8 | 61 ± 19 | 0.94 |
| Quartiles | ||||||
|---|---|---|---|---|---|---|
| Variable | Min | 25 | 75 | Max | p-Value | |
| 75% IDeg | BG (mmol/L) BG (mg/dL) | 6.7 ± 0.7 † 120 ± 13 | 8.4 ± 0.6 150 ± 11 | 10.5 ± 0.5 189 ± 9 | 13.9 ± 2.6 † 250 ± 46 | 0.03 |
| CHO (g) | 54 (18–73) | 44 (33–72) | 36 (18–54) | 0 (0–18) | ||
| 100% IDeg | BG (mmol/L) BG (mg/dL) | 7.3 ± 0.8 * 131 ± 15 | 8.7 ± 0.3 156 ± 6 | 10.2 ± 0.5 * 184 ± 10 | 12.4 ± 1.7 223 ± 30 | 0.03 |
| CHO (g) | 62 ± 36 | 40 ± 30 | 22 ± 25 | 30 ± 35 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moser, O.; Eckstein, M.L.; Mueller, A.; Birnbaumer, P.; Aberer, F.; Koehler, G.; Sourij, C.; Kojzar, H.; Pferschy, P.; Dietz, P.; et al. Pre-Exercise Blood Glucose Levels Determine the Amount of Orally Administered Carbohydrates during Physical Exercise in Individuals with Type 1 Diabetes—A Randomized Cross-Over Trial. Nutrients 2019, 11, 1287. https://doi.org/10.3390/nu11061287
Moser O, Eckstein ML, Mueller A, Birnbaumer P, Aberer F, Koehler G, Sourij C, Kojzar H, Pferschy P, Dietz P, et al. Pre-Exercise Blood Glucose Levels Determine the Amount of Orally Administered Carbohydrates during Physical Exercise in Individuals with Type 1 Diabetes—A Randomized Cross-Over Trial. Nutrients. 2019; 11(6):1287. https://doi.org/10.3390/nu11061287
Chicago/Turabian StyleMoser, Othmar, Max L. Eckstein, Alexander Mueller, Philipp Birnbaumer, Felix Aberer, Gerd Koehler, Caren Sourij, Harald Kojzar, Peter Pferschy, Pavel Dietz, and et al. 2019. "Pre-Exercise Blood Glucose Levels Determine the Amount of Orally Administered Carbohydrates during Physical Exercise in Individuals with Type 1 Diabetes—A Randomized Cross-Over Trial" Nutrients 11, no. 6: 1287. https://doi.org/10.3390/nu11061287