Disclosing and Reporting Practice Errors by Nurses in Residential Long-Term Care Settings: A Systematic Review

 ,
,  ,
, 

Abstract
:1. Introduction
Background
2. Materials and Methods
2.1. Design
2.2. Search Strategy and Sata Collection
2.3. Articles’ Selection and Quality Appraisal
2.4. Data Extraction and Analysis According to the Theoretical Framework
3. Results
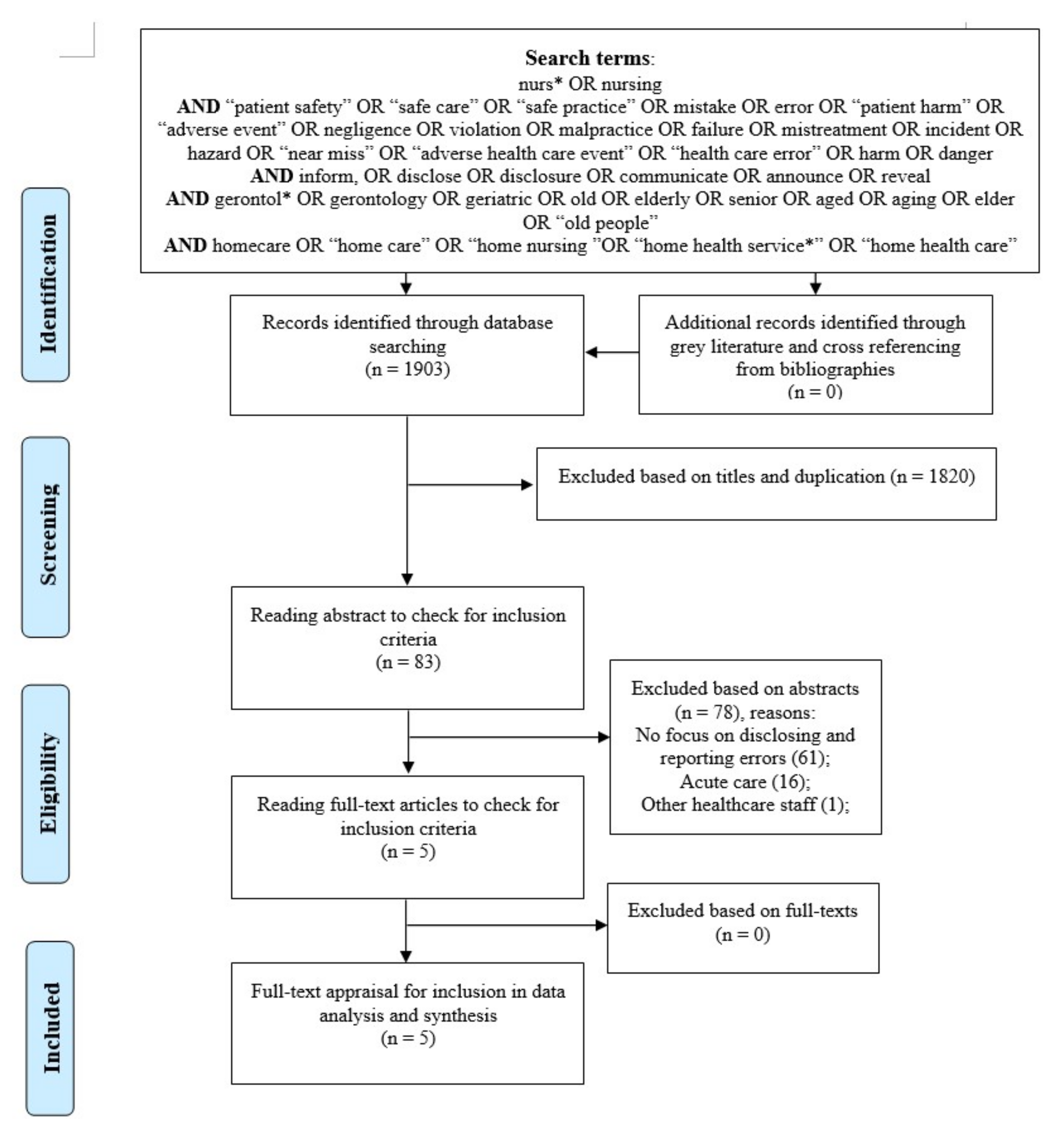
3.1. Search and Study Selections
3.2. General Sescription of the Selected Studies
3.3. Categorization of the Review Findings to the Vincent’s Framework
3.3.1. Patient
3.3.2. Healthcare Provider
3.3.3. Task
3.3.4. Work Environment
3.3.5. Organization and Management
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (WHO). National Institute on Aging National Institutes of Health. 2011. Available online: https://www.who.int/ageing/publications/global_health.pdf (accessed on 25 February 2019).
- Kingston, A.; Robinson, L.; Booth, H.; Knapp, M.; Jagger, C.; MODEM project. Projections of multi-morbidity in the older population in England to 2035: Estimates from the Population Ageing and Care Simulation (PACSim) model. Age Ageing 2018, 47, 374–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paal, P.; Brandstötter, C.; Lorenzl, S.; Larkin, P.; Elsner, F. Postgraduate palliative care education for all healthcare providers in Europe: Results from an EAPC survey. Palliat Support. Care 2019, 17, 495–506. [Google Scholar] [CrossRef] [PubMed]
- European Observatory on Health Systems and Policies. Sustainable health financing with an ageing population: Will population ageing lead to uncontrolled health expenditure growth? 2019. Available online: https://apps.who.int/iris/bitstream/handle/10665/329382/19978073-eng.pdf?sequence=1&isAllowed=y (accessed on 25 February 2020).
- World Health Organization (WHO). WHO Guidelines on Integrated Care for Older People (ICOPE). 2017. Available online: https://www.who.int/ageing/publications/guidelines-icope/en/ (accessed on 25 February 2020).
- Braithwaite, J.; Testa, L.; Lamprell, G.; Herkes, J.; Ludlow, K.; McPherson, E.; Campbell, M.; Holt, J. Built to last? The sustainability of health system improvements, interventions and change strategies: A study protocol for a systematic review. BMJ Open 2017, 7, e018568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortimer, F.; Isherwood, J.; Wilkinson, A.; Vaux, E. Sustainability in quality improvement: Redefining value. Future Healthc J. 2018, 5, 88–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Patient Safety. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/patient-safety (accessed on 26 February 2020).
- Mitchell, P.H. Defining Patient Safety and Quality Care. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Chapter 1; Hughes, R.G., Ed.; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2008. Available online: https://www.ncbi.nlm.nih.gov/books/NBK2681/ (accessed on 25 March 2020).
- World Health Organization (WHO). 10 Facts on Patient Safety. 2019. Available online: https://www.who.int/features/factfiles/patient_safety/en/ (accessed on 26 February 2020).
- United Nations. Sustainable development goals: Goal 3: Ensure healthy lives and promote well-being for all at all ages. 2020. Available online: https://www.un.org/sustainabledevelopment/health/ (accessed on 17 March 2020).
- Storch, J.; Curry, C.G.; Stevenson, L.; Macdonald, M.; Lang, A. Ethics and safety in home care: Perspectives on home support workers. Nurs Lead. (Toronto) 2014, 27, 76–96. [Google Scholar] [CrossRef] [PubMed]
- Simmons, S.F.; Schnelle, J.F.; Sathe, N.A.; Slagle, J.M.; Stevenson, D.G.; Carlo, M.E.; McPheeters, M.L. Defining Safety in the Nursing Home Setting: Implications for Future Research. J. Am. Med. Dir. Assoc. 2016, 17, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Agency for Healthcare Research and Quality, Patient Safety Network. Long-term Care and Patient Safety. Available online: https://psnet.ahrq.gov/primer/long-term-care-and-patient-safety (accessed on 1 January 2020).
- Ferrah, N.; Lovell, J.J.; Ibrahim, J.E. Systematic Review of the Prevalence of Medication Errors Resulting in Hospitalization and Death of Nursing Home Residents. J. Am. Geriatr. Soc. 2017, 65, 433–442. [Google Scholar] [CrossRef]
- Storms, H.; Marquet, K.; Aertgeerts, B.; Claes, N. Prevalence of inappropriate medication use in residential long-term care facilities for the elderly: A systematic review. Eur. J. Gen. Pr. 2017, 23, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Brauner, D.; Werner, R.M.; Shippee, T.P.; Cursio, J.; Sharma, H.; Konetzka, R.T. Does Nursing Home Compare Reflect Patient Safety In Nursing Homes? Health Aff. (Millwood) 2018, 37, 1770–1778. [Google Scholar] [CrossRef] [Green Version]
- Renz, S.M.; Carrington, J.M. Nurse-Physician Communication in Long-Term Care: Literature Review. J. Gerontol. Nurs. 2016, 1–8. [Google Scholar] [CrossRef]
- Jordan, S.; Banner, T.; Gabe-Walters, M.; Mikhail, J.M.; Panes, G.; Round, J.; Snelgrove, S.; Storey, M.; Hughes, D.; Medicines’ Management Group, Swansea University. Nurse-led medicines’ monitoring in care homes, implementing the Adverse Drug Reaction (ADRe) Profile improvement initiative for mental health medicines: An observational and interview study. PLoS ONE 2019, 14, e0220885. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.; Logan, P.A.; Panes, G.; Vaismoradi, M.; Hughes, D. Adverse Drug Reactions, Power, Harm Reduction, Regulation and the ADRe Profiles. Pharmacy (Basel) 2018, 6, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, L.M.; Capezuti, E.; Ouslander, J.G. Reporting near-miss events in nursing homes. Nurs. Outlook 2006, 54, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Tariq, A.; Georgiou, A.; Westbrook, J. Medication incident reporting in residential aged care facilities: Limitations and risks to residents’ safety. BMC Geriatr. 2012, 12, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, Z.R.; Hughes, R.G. Error Reporting and Disclosure. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Chapter 35; Hughes, R.G., Ed.; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2008. Available online: http://www.ncbi.nlm.nih.gov/books/NBK2652 (accessed on 17 December 2019).
- Steven, A.; Tella, S.; Turunen, H.; Flores Vizcaya-Moreno, M.; Pérez-Cañaveras, R.M.; Porras, J.; Bagnasco, A.; Sasso, L.; Myhre, K.; Sara-aho, A.; et al. Shared learning from national to international contexts: A research and innovation collaboration to enhance education for patient safety. J. Res. Nurs. 2019, 24, 149–164. [Google Scholar] [CrossRef] [Green Version]
- Tricarico, P.; Castriotta, L.; Battistella, C.; Bellomo, F.; Cattani, G.; Grillone, L.; Degan, S.; De Corti, D.; Brusaferro, S. Professional attitudes toward incident reporting: Can we measure and compare improvements in patient safety culture? Int. J. Qual. Health Care 2017, 29, 243–249. [Google Scholar] [CrossRef] [Green Version]
- Cheung, K.L.; Ten Klooster, P.M.; Smit, C.; de Vries, H.; Pieterse, M.E. The impact of non-response bias due to sampling in public health studies: A comparison of voluntary versus mandatory recruitment in a Dutch national survey on adolescent health. BMC Public Health 2017, 17, 276. [Google Scholar] [CrossRef] [Green Version]
- Vrbnjak, D.; Denieffe, S.; O’Gorman, C.; Pajnkihar, M. Barriers to reporting medication errors and near misses among nurses: A systematic review. Int. J. Nurs. Stud. 2016, 63, 162–178. [Google Scholar] [CrossRef]
- Khan, A.; Spector, N.D.; Baird, J.D.; Ashland, M.; Starmer, A.J.; Rosenbluth, G.; Garcia, B.M.; Litterer, K.P.; Rogers, J.E.; Dalal, A.K.; et al. Patient safety after implementation of a coproduced family centered communication programme: Multicenter before and after intervention study. BMJ 2018, 363, k4764. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Reporting and learning systems for medication errors: The role of pharmacovigilance centres. 2014. Available online: https://www.who.int/medicines/areas/quality_safety/safety_efficacy/emp_mes/en/ (accessed on 26 February 2020).
- Anderson, J.E.; Kodate, N.; Walters, R.; Dodds, A. Can incident reporting improve safety? Healthcare practitioners’ views of the effectiveness of incident reporting. Int. J. Qual. Health Care 2013, 25, 141–150. [Google Scholar] [CrossRef] [Green Version]
- Macrae, C. The problem with incident reporting. BMJ Qual. Saf. 2016, 25, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rangraz Jeddi, F.; Akbari, H.; Rasoli, S. Older people home care through electronic health records: Functions, data elements and security needs. Contemp. Nurse 2016, 52, 352–365. [Google Scholar] [CrossRef] [PubMed]
- Johansson-Pajala, R.-M.; Jorsäter Blomgren, K.; Bastholm-Rahmner, P.; Fastbom, J.; Martin, L. Nurses in municipal care of the elderly act as pharmacovigilant intermediaries: A qualitative study of medication management. Scand. J. Prim. Health Care 2016, 34, 37–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dirik, H.F.; Samur, M.; Seren Intepeler, S.; Hewison, A. Nurses’ identification and reporting of medication errors. J. Clin. Nurs. 2019, 28, 931–938. [Google Scholar] [CrossRef] [Green Version]
- Chapuis, C.; Chanoine, S.; Colombet, L.; Calvino-Gunther, S.; Tournegros, C.; Terzi, N.; Bedouch, P.; Schwebel, C. Interprofessional safety reporting and review of adverse events and medication errors in critical care. Clin. Risk Manag. 2019, 15, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Sarvadikar, A.; Prescott, G.; Williams, D. Attitudes to reporting medication error among differing healthcare professionals. Eur. J. Clin. Pharmacol. 2010, 66, 843–853. [Google Scholar] [CrossRef] [Green Version]
- Choe, K.; Kang, H.; Lee, A. Barriers to ethical nursing practice for older adults in long-term care facilities. J. Clin. Nurs. 2018, 27, 1063–1072. [Google Scholar] [CrossRef]
- Tuinman, A.; de Greef, M.H.G.; Krijnen, W.P.; Paans, W.; Roodbol, P.F. Accuracy of documentation in the nursing care plan in long-term institutional care. Geriatr. Nurs. 2017, 38, 578–583. [Google Scholar] [CrossRef]
- Hewitt, T.; Chreim, S.; Forster, A. Sociocultural Factors Influencing Incident Reporting Among Physicians and Nurses: Understanding Frames Underlying Self- and Peer-Reporting Practices. J. Patient Saf. 2017, 13, 129–137. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1; John Wiley & Sons: Chichester, UK, 2011; Available online: http://handbook-5-1.cochrane.org/ (accessed on 17 December 2019).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.; Harden, A.; Oakley, A.; Oliver, S.; Sutcliffe, K.; Rees, R.; Brunton, G.; Kavanagh, J. Integrating qualitative research with trials in systematic reviews. BMJ 2004, 328, 1010–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The UK EQUATOR Centre. Enhancing the QUAlity and Transparency of Health Research (EQUATOR). Available online: http://www.equator-network.org/ (accessed on 17 December 2019).
- Preferred reporting items for systematic review and meta-analysis protocols (PRISMA). Available online: http://prisma-statement.org/PRISMAStatement/PRISMAStatement (accessed on 17 December 2019).
- Vincent, C.; Taylor-Adams, S.; Stanhope, N. Framework for analysing risk and safety in clinical medicine. BMJ 1998, 316, 1154–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reason, J. Understanding adverse events: Human factors. Qual. Health Care 1995, 4, 80–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, C.; Burnett, S.; Carthey, J. Safety measurement and monitoring in healthcare: A framework to guide clinical teams and healthcare organisations in maintaining safety. BMJ Qual. Saf. 2014, 23, 670–677. [Google Scholar] [CrossRef] [Green Version]
- Hěib, Z.; Vychytil, P.; Marx, D. Adverse event reporting in Czech long-term care facilities. Int. J. Qual. Health Care 2013, 25, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Wagner, L.M.; Harkness, K.; Hébert, P.C.; Gallagher, T.H. Nurses’ perceptions of error reporting and disclosure in nursing homes. J. Nurs. Care Qual. 2012, 27, 63–69. [Google Scholar] [CrossRef] [Green Version]
- Winsvold Prang, I.; Jelsness-Jørgensen, L.-P. Should I report? A qualitative study of barriers to incident reporting among nurses working in nursing homes. Geriatr. Nurs. 2014, 35, 441–447. [Google Scholar] [CrossRef]
- Berland, A.; Bentsen, S.B. Medication errors in home care: A qualitative focus group study. J. Clin. Nurs. 2017, 26, 3734–3741. [Google Scholar] [CrossRef]
- Wagner, L.M.; Driscoll, L.; Darlington, J.L.; Flores, V.; Kim, J.; Melino, K.; Patel, H.D.; Spetz, J. Nurses’ Communication of Safety Events to Nursing Home Residents and Families. J. Gerontol. Nurs. 2018, 44, 25–32. [Google Scholar] [CrossRef]
- Bjornsdottir, K. ‘I try to make a net around each patient’: Home care nursing as relational practice. Scand. J. Caring Sci. 2018, 32, 177–185. [Google Scholar] [CrossRef]
- Cunningham, C.E.; Hutchings, T.; Henderson, J.; Rimas, H.; Chen, Y. Modeling the hospital safety partnership preferences of patients and their families: A discrete choice conjoint experiment. Patient Prefer. Adherence 2016, 10, 1359–1372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koskenniemi, J.; Leino-Kilpi, H.; Suhonen, R. Manifestation of respect in the care of older patients in long-term care settings. Scand. J. Caring Sci. 2015, 29, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Prouty, C.D.; Foglia, M.B.; Gallagher, T.H. Patients’ experiences with disclosure of a large-scale adverse event. J. Clin. Ethics 2013, 24, 353–363. [Google Scholar] [PubMed]
- Dreyer, A.; Strom, A. Involving relatives in consultations for patients with long-term illnesses: Nurses and physicians’ experiences. Nurs. Ethics 2019, 26, 2124–2134. [Google Scholar] [CrossRef]
- Vaismoradi, M.; Jordan, S.; Kangasniemi, M. Patient participation in patient safety and nursing input—A systematic review. J. Clin. Nurs. 2015, 24, 627–639. [Google Scholar] [CrossRef] [Green Version]
- McLennan, S.R.; Diebold, M.; Rich, L.E.; Elger, B.S. Nurses’ perspectives regarding the disclosure of errors to patients: A qualitative study. Int. J. Nurs. Stud. 2016, 54, 16–22. [Google Scholar] [CrossRef]
- Rutledge, D.N.; Retrosi, T.; Ostrowski, G. Barriers to medication error reporting among hospital nurses. J. Clin. Nurs. 2018, 27, 1941–1949. [Google Scholar] [CrossRef]
- Welsh, D.; Zephyr, D.; Pfeifle, A.L.; Carr, D.E.; Fink, J.L., III; Jones, M. Development of the Barriers to Error Disclosure Assessment Tool. J. Patient Saf. 2017. [Google Scholar] [CrossRef] [Green Version]
- Newman, A.R. Nurses’ Perceptions of Diagnosis and Prognosis-Related Communication: An Integrative Review. Cancer Nurs. 2016, 39, E48–E60. [Google Scholar] [CrossRef]
- Amaniyan, S.; Faldaas, B.O.; Logan, P.A.; Vaismoradi, M. Learning from Patient Safety Incidents in the Emergency Department: A Systematic Review. J. Emerg. Med. 2019. [Google Scholar] [CrossRef]
- Barry, T.T.; Longacre, M.; Carney, K.O.S.; Patterson, S. Team inclusion and empowerment among nursing staff in long-term care. Geriatr. Nurs. 2019, 40, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Tajabadi, A.; Ahmadi, F.; Sadooghi Asl, A.; Vaismoradi, M. Unsafe nursing documentation: A qualitative content analysis. Nurs. Ethics 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaismoradi, M.; Bondas, T.; Salsali, M.; Jasper, M.; Turunen, H. Facilitating safe care: A qualitative study of Iranian nurse leaders. J. Nurs. Manag. 2014, 22, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.Y.; Pyo, J.; Ock, M.; Lee, S.-I. Nurses’ Perceptions Regarding Disclosure of Patient Safety Incidents in Korea: A Qualitative Study. Asian Nurs. Res. (Korean Soc. Nurs. Sci.) 2019, 13, 200–208. [Google Scholar] [CrossRef] [Green Version]
- Kangasniemi, M.; Vaismoradi, M.; Jasper, M.; Turunen, H. Ethical issues in patient safety: Implications for nursing management. Nurs. Ethics 2013, 20, 904–916. [Google Scholar] [CrossRef]
- Vaismoradi, M.; Griffiths, P.; Turunen, H.; Jordan, S. Transformational leadership in nursing and medication safety education: A discussion paper. J. Nurs. Manag. 2016, 24, 970–980. [Google Scholar] [CrossRef] [Green Version]
- Byju, A.S.; Mayo, K. Medical error in the care of the unrepresented: Disclosure and apology for a vulnerable patient population. J. Med. Ethics 2019, 45, 821–823. [Google Scholar] [CrossRef]
- Gardner, A.K.; Lim, G.; Minard, C.G.; Guffey, D.; Pillow, M.T. A Cross-Specialty Examination of Resident Error Disclosure and Communication Skills Using Simulation. J. Grad. Med. Educ. 2018, 10, 438–441. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.W.; Myung, S.J.; Eo, E.K.; Chang, Y. Improving disclosure of medical error through educational program as a first step toward patient safety. BMC Med. Educ. 2017, 17, 52. [Google Scholar] [CrossRef] [Green Version]
- Leone, D.; Lamiani, G.; Vegni, E.; Larson, S.; Roter, D.L. Error disclosure and family members’ reactions: Does the type of error really matter? Patient Educ. Couns. 2015, 98, 446–452. [Google Scholar] [CrossRef]
- Perez, B.; Knych, S.A.; Weaver, S.J.; Liberman, A.; Abel, E.M.; Oetjen, D.; Wan, T.T.H. Understanding the barriers to physician error reporting and disclosure: A systemic approach to a systemic problem. J. Patient Saf. 2014, 10, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Øygard, S.H.; Andersen, J.R.; Sandvoll, A.M.; Ytrehus, S. Manglande registrering av fall i sjukeheim. Sykepleien Forskning. Sykepl. Forsk. 2017, 12, e-62446. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Database/Articles from 2010–2019 | Total in Each Database | Selected Based on Title Reading | Selected Based on Abstract Reading | Selected Based on Full-Text Appraisal |
|---|---|---|---|---|
| PubMed (including Medline) | 77 | 39 | 0 | 0 |
| Scopus | 826 | 23 | 4 | 4 |
| Cinahl | 347 | 6 | 2 | 1 |
| Embase | 157 | 7 | 0 | 0 |
| Medes (Spanish) | 2 | 1 | 1 | 0 |
| Cuiden (Spanish) | 474 | 5 | 5 | 0 |
| Norart (Nordic) | 6 | 0 | 0 | 0 |
| SveMed+ (Nordic) | 14 | 2 | 2 | 0 |
| Manual search/backtracking references | 0 | 0 | 0 | 0 |
| Total | 1903 | 83 | 14 | 5 |
| Author, Year, Country | Aim | Method | Setting and Sample | Reported Outcome/Findings | Structure Used for Error Disclosure and Reporting | Quality Appraisal Instrument and Score |
|---|---|---|---|---|---|---|
| Wagner et al., 2012, Canada [49] | To describe nurses’ perceptions of error disclosure in nursing homes. | Cross-sectional email survey | 1180 nurses working in nursing homes; no data on the number of nursing homes with a response rate of 50% | Relationships between tendency to disclosing errors and previous experience of error disclosure were reported. | Resident, nurse, error severity/outcome, and institutional culture | STROBE, 22 |
| Hěib et al., 2013, Czech Republic [48] | To describe the processes used for reporting adverse events in long-term care settings. | Prospective cohort study | 111 long-term facilities and 11 in-person visits to facilities with a response rate of 100% | 37% of visited facilities had no policy for error reporting. | Definition of adverse events, responsibilities, reporting, and analyzing | STROBE, 24, |
| Winsvold Prang and Jelsness-Jørgense, 2014, Norway [50] | To explore barriers to reporting errors and incidents in nursing homes. | Qualitative design using thematic analysis | 13 nurses working in 17 nursing homes | Culture of error reporting and disclosure was not established. | Organizational and individual barriers | COREQ, 24 |
| Berland and Bentsen, 2017 Norway [51] | To explore nurses’ experiences of patient safety, medication errors, and disclosing errors in care homes. | Qualitative design using content analysis | 20 nurses from 2 municipalities | Necessity of openness and routines regarding reporting errors was not always understood. | Inductive approach | COREQ, 21 |
| Wagner et al., 2018, USA [52] | To educate nurses on how to disclose patient safety events to residents and family members using a structured communication tool. | Mixed-methods | 77 nurses from 6 nursing homes; 9 interviews in 1 nursing home | Process and structure of communicating errors to residents and families were lacking. | Anticipate, listen, empathize, explain, and follow up | GRAMMS, 9 |
| Author, Year Vincent’s Framework | Wagner et al., 2012 [49] | Hěib et al., 2013 [48] | Winsvold Prang and Jelsness-Jørgensen, 2014 [50] | Berland and Bentsen, 2017 [51] | Wagner et al., 2018 [52] |
|---|---|---|---|---|---|
| Patient | Damaging residents’ trust in nurses’ competencies and getting sued; residents’ and families’ understandings of errors. | No data | No data | No data | Clear and understandable language and without jargon/medical terminology for communication of errors to residents and families; discussing preventive measures with residents and families; listening to residents/families and allowing time for their reflection and feedback; use of empathetic statements without becoming defensive during communication. |
| Healthcare provider | Personal attitude regarding the significance of errors; discussing errors and near misses with colleagues; necessity of knowing about errors; knowledge on how to disclose errors; interest in receiving education on error disclosure; more error disclosure by well-educated nurses; history of reporting errors of varying severity; more disclosure of serious errors. | No data | Prior experience with reporting errors; knowledge and confidence in the digital reporting system; personal belief in the sensitivity and seriousness of errors. | Being good at disclosing errors | Feeling responsible for errors; being in favor of fully disclosing error, providing details, and discussing prevention; being confident in communicating errors to residents and families. |
| Task | No data | No data | Heavy work obligations and lack of time to report errors. | No data | Continuity and closeness of monitoring resident after committing error. |
| Work environment | Failure in the care system as the cause of errors; receiving support to cope with the associated stress of errors. | No data | General negative attitudes in the system towards error reporting; focus on reporting errors in daily practice; | Openness to disclose and communicate errors to other colleagues, physicians, residents and relatives. | No data |
| Organization and management | Nurse leader as responsible for disclosing errors to family and residents; reporting system available; adequacy of mechanisms to inform nurses about errors. | Need for internal policies on error reporting and cause analysis; requesting staff to report errors; direct reporting or via superiors; standardized reporting systems as paper of electronic formats. | Unclear routines for handling error reports; no information and feedback about the consequences of reported errors, such as improvement of routines and surveillance; previous negative feedback to reported errors; being encouraged by leaders to report errors selectively; protection of anonymity of reporting; fear of conflict with others and reprimand; level of sensitivity and seriousness of error from the system’s perspective. | Devising initiatives by nurse leaders to disclose medication errors. | Being concerned about getting reprimanded and damaging professional reputation. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaismoradi, M.; Vizcaya-Moreno, F.; Jordan, S.; Gåre Kymre, I.; Kangasniemi, M. Disclosing and Reporting Practice Errors by Nurses in Residential Long-Term Care Settings: A Systematic Review. Sustainability 2020, 12, 2630. https://doi.org/10.3390/su12072630
Vaismoradi M, Vizcaya-Moreno F, Jordan S, Gåre Kymre I, Kangasniemi M. Disclosing and Reporting Practice Errors by Nurses in Residential Long-Term Care Settings: A Systematic Review. Sustainability. 2020; 12(7):2630. https://doi.org/10.3390/su12072630
Chicago/Turabian StyleVaismoradi, Mojtaba, Flores Vizcaya-Moreno, Sue Jordan, Ingjerd Gåre Kymre, and Mari Kangasniemi. 2020. "Disclosing and Reporting Practice Errors by Nurses in Residential Long-Term Care Settings: A Systematic Review" Sustainability 12, no. 7: 2630. https://doi.org/10.3390/su12072630