

Tooth Loss, Cognitive Impairment and Fall Risk: A Cross-Sectional Study of Older Adults in Rural Thailand

 , and
, and 
Abstract
:
1. Introduction
2. Materials and Methods
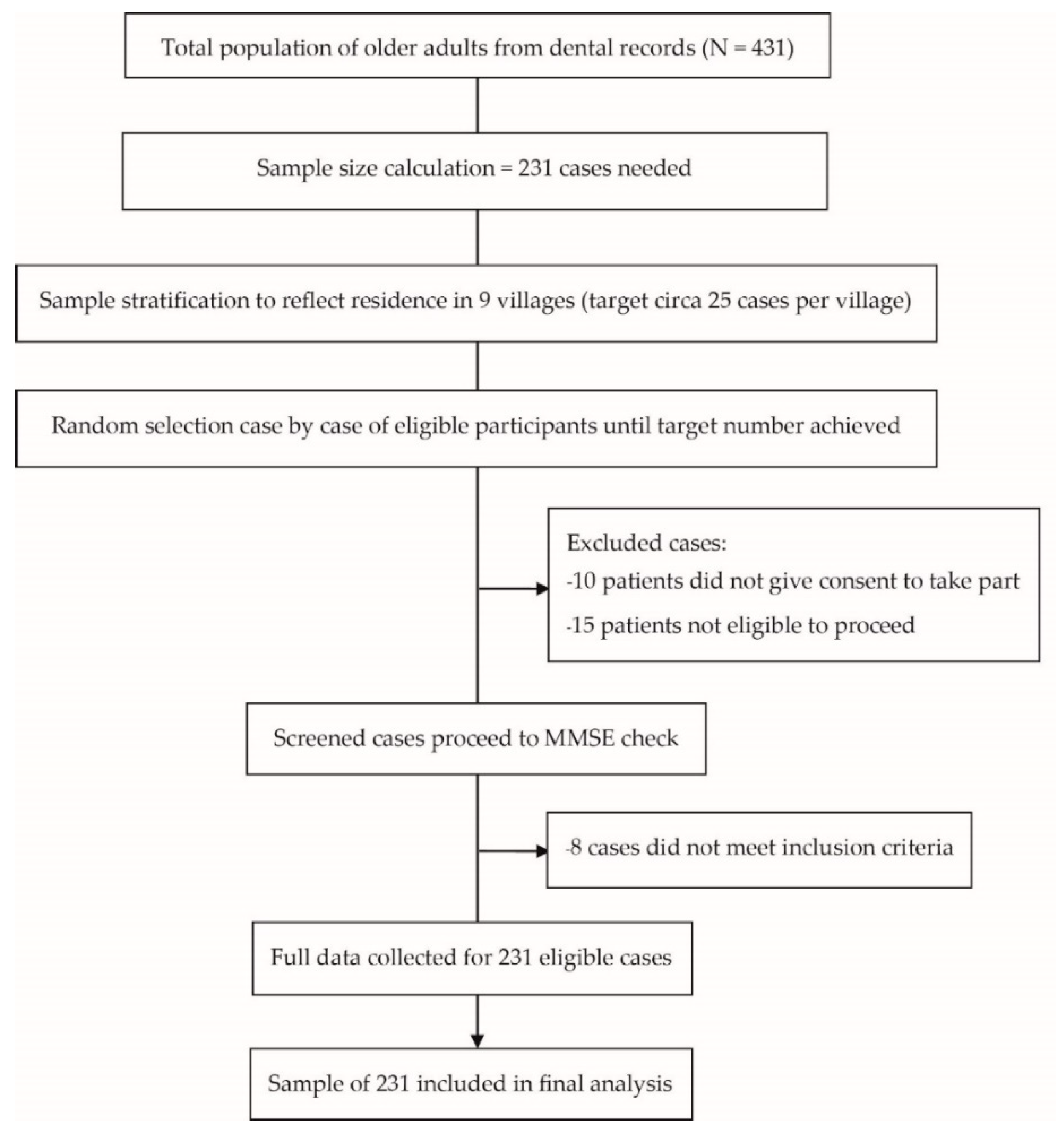
2.1. Research Design
2.2. Statistical Analysis
3. Results
3.1. Characteristics of General and Dental Status of Older Adults
3.2. Factors Predicting Cognitive Impairment in Older Adults
3.3. Association between Cognitive Function and Fall Risk
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, X.; Clark, J.J.; Chen, H.; Naorungroj, S. Cognitive impairment, oral self-care function and dental caries severity in community-dwelling older adults. Gerodontology 2015, 32, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Monachan, D.; Vargese, S.S.; Johny, V.; Mathew, E. Risk of Fall among Older Adults and its Association with Cognitive Impairment in a Semi-Urban Community. Indian J. Community Med. 2020, 45, 463–466. [Google Scholar]
- Fang, W.L.; Jiang, M.J.; Gu, B.B.; Wei, Y.M.; Fan, S.N.; Liao, W.; Zheng, Y.Q.; Liao, S.W.; Xiong, Y.; Li, Y.; et al. Tooth loss as a risk factor for dementia: Systematic review and meta-analysis of 21 observational studies. BMC Psychiatry 2018, 18, 345. [Google Scholar] [CrossRef] [Green Version]
- Dibello, V.; Zupo, R.; Sardone, R.; Lozupone, M.; Castellana, F.; Dibello, A.; Daniele, A.; De Pergola, G.; Bortone, I.; Lampignano, L.; et al. Oral frailty and its determinants in older age: A systematic review. Lancet Healthy Longev. 2021, 2, e507–e520. [Google Scholar] [CrossRef]
- Luo, J.; Wu, B.; Zhao, Q.; Guo, Q.; Meng, H.; Yu, L.; Zheng, L.; Hong, Z.; Ding, D. Association between tooth loss and cognitive function among 3063 Chinese older adults: A community-based study. PLoS ONE 2015, 10, e0120986. [Google Scholar] [CrossRef] [Green Version]
- Minn, Y.-K.; Suk, S.-H.; Park, H.; Cheong, J.-S.; Yang, H.; Lee, S.; Do, S.-Y.; Kang, J.-S. Tooth loss is associated with brain white matter change and silent infarction among adults without dementia and stroke. J. Korean Med. Sci. 2013, 28, 929–933. [Google Scholar] [CrossRef] [Green Version]
- Ha, V.T.; Nguyen, T.N.; Nguyen, T.X.; Nguyen, H.T.T.; Nguyen, T.T.H.; Nguyen, A.T.; Pham, T.; Vu, H.T.T. Prevalence and Factors Associated with Falls among Older Outpatients. Int. J. Environ. Res. Public Health 2021, 18, 4041. [Google Scholar] [CrossRef]
- World Health Organization. WHO Country Cooperation Strategy Thailand, 2012–2016; World Health Organization. Regional Office for South-East Asia: New Delhi, India, 2012.
- Srinarupat, J.; Oshiro, A.; Zaitsu, T.; Prasertsom, P.; Niyomsilp, K.; Kawaguchi, Y.; Aida, J. Inequalities in Periodontal Disease According to Insurance Schemes in Thailand. Int. J. Environ. Res. Public Health 2021, 18, 5945. [Google Scholar] [CrossRef]
- Nazir, M.; Al-Ansari, A.; Al-Khalifa, K.; Alhareky, M.; Gaffar, B.; Almas, K. Global Prevalence of Periodontal Disease and Lack of Its Surveillance. Sci. World J. 2020, 2020, 2146160. [Google Scholar] [CrossRef]
- Pockpa, Z.A.D.; Struillou, X.; Kone, D.; Mobio, G.S.; Soueidan, A.; Badran, Z. Periodontal Diseases and Age-Related Macular Degeneration: Is There a Link? A Review. Perm. J. 2019, 23, 18.260. [Google Scholar] [CrossRef]
- Tanglakmankhong, K.; Hampstead, B.M.; Ploutz-Snyder, R.J.; Potempa, K. Cognitive screening assessment in Thai older adults: A prospective study of the reliability and validity of the Abbreviated Mental Test. J. Health Res. 2022, 36, 99–109. [Google Scholar] [CrossRef]
- Tanglakmankhong, K.; Hampstead, B.M.; Ploutz-Snyder, R.J.; Potempa, K. Does the Abbreviated Mental Test Accurately Predict Cognitive Impairment in Thai Older Adults? A Retrospective Study. Pac. Rim Int. J. Nurs. Res. Thail. 2021, 25, 23–33. [Google Scholar]
- Zaudig, M. A new systematic method of measurement and diagnosis of “mild cognitive impairment” and dementia according to ICD-10 and DSM-III-R criteria. Int. Psychogeriatr. 1992, 4 (Suppl. S2), 203–219. [Google Scholar] [CrossRef]
- Krejcie, R.V.; Morgan, D.W. Determining sample size for research activities. Educ. Psychol. Meas. 1970, 30, 607–610. [Google Scholar] [CrossRef]
- Aung, T.N.N.; Moolphate, S.; Koyanagi, Y.; Angkurawaranon, C.; Supakankunti, S.; Yuasa, M.; Aung, M.N. Determinants of Health-Related Quality of Life Among Community-Dwelling Thai Older Adults in Chiang Mai, Northern Thailand. Risk Manag. Healthc. Policy 2022, 15, 1761–1774. [Google Scholar] [CrossRef]
- Chatrchaiwiwatana, S. Dental caries and periodontitis associated with betel quid chewing: Analysis of two data sets. J. Med. Assoc. Thai 2006, 89, 1004–1011. [Google Scholar]
- Ainamo, J.; Barmes, D.; Beagrie, G.; Cutress, T.; Martin, J.; Sardo-Infirri, J. Development of the World Health Organization (WHO) Community Periodontal Index of Treatment Needs (CPITN). Int. Dent. J. 1982, 32, 281–291. [Google Scholar]
- World Health Organization. Oral Health Surveys: Basic Methods; World Health Organization: Geneva, Switzerland, 2013.
- Sermsuti-Anuwat, N.; Piyakhunakorn, P. Association Between Oral Health Literacy and Number of Remaining Teeth Among the Thai Elderly: A Cross-Sectional Study. Clin. Cosmet. Investig. Dent. 2021, 13, 113–119. [Google Scholar] [CrossRef]
- Okamoto, N.; Morikawa, M.; Okamoto, K.; Habu, N.; Iwamoto, J.; Tomioka, K.; Saeki, K.; Yanagi, M.; Amano, N.; Kurumatani, N. Relationship of tooth loss to mild memory impairment and cognitive impairment: Findings from the Fujiwara-kyo study. Behav. Brain Funct. 2010, 6, 77. [Google Scholar] [CrossRef] [Green Version]
- Filley, C.M.; Fields, R.D. White matter and cognition: Making the connection. J. Neurophysiol. 2016, 116, 2093–2104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akashi, M.; Tanaka, K.; Kusumoto, J.; Furudoi, S.; Hosoda, K.; Komori, T. Brain Abscess Potentially Resulting from Odontogenic Focus: Report of Three Cases and a Literature Review. J. Maxillofac. Oral Surg. 2017, 16, 58–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Liu, S.Y.; Hossaini-Zadeh, M.; Pogrel, M.A. Brain abscess potentially secondary to odontogenic infection: Case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, e108–e111. [Google Scholar] [CrossRef] [PubMed]
- Scolari, M.; Seidl-Rathkopf, K.N.; Kastner, S. Functions of the human frontoparietal attention network: Evidence from neuroimaging. Curr. Opin. Behav. Sci. 2015, 1, 32–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickerson, B.C.; Salat, D.H.; Bates, J.F.; Atiya, M.; Killiany, R.J.; Greve, D.N.; Dale, A.M.; Stern, C.E.; Blacker, D.; Albert, M.S.; et al. Medial temporal lobe function and structure in mild cognitive impairment. Ann. Neurol. 2004, 56, 27–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riviere, G.R.; Riviere, K.H.; Smith, K.S. Molecular and immunological evidence of oral Treponema in the human brain and their association with Alzheimer’s disease. Oral Microbiol. Immunol. 2002, 17, 113–118. [Google Scholar] [CrossRef]
- Wang, X.; Hu, J.; Jiang, Q. Tooth Loss-Associated Mechanisms That Negatively Affect Cognitive Function: A Systematic Review of Animal Experiments Based on Occlusal Support Loss and Cognitive Impairment. Front. Neurosci. 2022, 16, 811335. [Google Scholar] [CrossRef]
- Monteiro, A.M.; Forte, P.; Carvalho, J.; Barbosa, T.M.; Morais, J.E. Relationship between fear of falling and balance factors in healthy elderly women: A confirmatory analysis. J. Women Aging 2021, 33, 57–69. [Google Scholar] [CrossRef]
- Polzer, I.; Schwahn, C.; Volzke, H.; Mundt, T.; Biffar, R. The association of tooth loss with all-cause and circulatory mortality. Is there a benefit of replaced teeth? A systematic review and meta-analysis. Clin. Oral Investig. 2012, 16, 333–351. [Google Scholar] [CrossRef]
- Mochida, Y.; Yamamoto, T.; Fuchida, S.; Aida, J.; Kondo, K. Does poor oral health status increase the risk of falls?: The JAGES Project Longitudinal Study. PLoS ONE 2018, 13, e0192251. [Google Scholar] [CrossRef] [Green Version]
- Tinetti, M.E.; Speechley, M.; Ginter, S.F. Risk factors for falls among elderly persons living in the community. N. Engl. J. Med. 1988, 319, 1701–1707. [Google Scholar] [CrossRef]
- Perini, G.; Cotta Ramusino, M.; Sinforiani, E.; Bernini, S.; Petrachi, R.; Costa, A. Cognitive impairment in depression: Recent advances and novel treatments. Neuropsychiatr. Dis. Treat. 2019, 15, 1249–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerritsen, A.E.; Allen, P.F.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H. Tooth loss and oral health-related quality of life: A systematic review and meta-analysis. Health Qual. Life Outcomes 2010, 8, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bednarczuk, G.; Rutkowska, I. Factors of balance determining the risk of falls in physically active women aged over 50 years. PeerJ 2022, 10, e12952. [Google Scholar] [CrossRef] [PubMed]
- Shur, N.F.; Creedon, L.; Skirrow, S.; Atherton, P.J.; MacDonald, I.A.; Lund, J.; Greenhaff, P.L. Age-related changes in muscle architecture and metabolism in humans: The likely contribution of physical inactivity to age-related functional decline. Ageing Res. Rev. 2021, 68, 101344. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.E.; Kim, N.Y.; Choi, C.H.; Chung, K.H. Association between Present Teeth and Muscle Strength in Older People in Korea. J. Pers. Med. 2022, 12, 1163. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | n | % |
|---|---|---|
| Gender | ||
| Female | 105 | 45.5 |
| Male | 126 | 54.5 |
| Age | ||
| 60–69 | 153 | 66.2 |
| ≥70 | 78 | 33.8 |
| Marital status | ||
| Married | 161 | 69.7 |
| Single/divorced/Widowed/Separated | 70 | 30.3 |
| Educational level | ||
| No schooling | 87 | 37.7 |
| Primary school | 41 | 17.7 |
| Higher than primary school | 103 | 44.6 |
| BMI (kg/m2) | ||
| Normal (≥25 to≤35) | 71 | 30.7 |
| Health risk (<25 or >35) | 160 | 69.3 |
| ADLs | ||
| <12 | 14 | 6.1 |
| ≥12 | 217 | 93.9 |
| Congenital disease | ||
| No | 149 | 64.5 |
| Yes | 82 | 35.5 |
| Betel nut chewing | ||
| Never | 181 | 78.7 |
| Been chewing betel nuts | 49 | 21.3 |
| Number of teeth lost | ||
| ≤16 teeth | 143 | 61.9 |
| >16 teeth | 88 | 38.1 |
| Number of decayed teeth | ||
| None | 182 | 78.8 |
| ≥1 tooth | 49 | 21.2 |
| Number of dental fillings | ||
| None | 206 | 89.2 |
| ≥1 tooth | 25 | 10.8 |
| Number of opposing post-canine tooth pairs | ||
| ≥7 | 197 | 85.3 |
| <7 | 34 | 14.7 |
| Calculus | ||
| Not present | 113 | 48.9 |
| Present | 118 | 51.1 |
| Factors | Cognitive Function Level | Crude OR (95% CI) | Adjusted OR (95% CI) | p-Value | |||
|---|---|---|---|---|---|---|---|
| Normal (n = 149) | Impaired (n = 82) | ||||||
| n | % | n | % | ||||
| Age | |||||||
| 60–69 | 110 | 71.9 | 43 | 28.1 | Ref | Ref | Ref |
| ≥70 | 39 | 50.0 | 39 | 50.0 | 0.39 (0.22–0.68) | 2.64 (1.25–5.57) | 0.010 |
| ADLs | |||||||
| ≥12 | 145 | 66.8 | 72 | 33.2 | Ref | Ref | Ref |
| <12 | 4 | 28.6 | 10 | 71.4 | 5.03 (1.52–16.60) | 4.89 (1.17–20.40) | 0.029 |
| Number of teeth lost | |||||||
| ≤16 teeth | 113 | 79.0 | 30 | 21.0 | Ref | Ref | Ref |
| >16 teeth | 36 | 40.9 | 52 | 59.1 | 5.44 (3.03–9.76) | 4.29 (2.06–8.91) | <0.001 |
| Cognitive Function | Fall Risk | Total | 95% CI | χ2 | p-Value | |
|---|---|---|---|---|---|---|
| High Risk | Low Risk | |||||
| n (%) | n (%) | |||||
| Impaired | 47 (74.6) | 16 (25.4) | 63 (100) | 2.63–9.60 | 26.13 | <0.001 |
| Normal | 62 (36.9) | 106 (63.1) | 168 (100) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turnbull, N.; Cherdsakul, P.; Chanaboon, S.; Hughes, D.; Tudpor, K. Tooth Loss, Cognitive Impairment and Fall Risk: A Cross-Sectional Study of Older Adults in Rural Thailand. Int. J. Environ. Res. Public Health 2022, 19, 16015. https://doi.org/10.3390/ijerph192316015
Turnbull N, Cherdsakul P, Chanaboon S, Hughes D, Tudpor K. Tooth Loss, Cognitive Impairment and Fall Risk: A Cross-Sectional Study of Older Adults in Rural Thailand. International Journal of Environmental Research and Public Health. 2022; 19(23):16015. https://doi.org/10.3390/ijerph192316015
Chicago/Turabian StyleTurnbull, Niruwan, Pichayasuda Cherdsakul, Sutin Chanaboon, David Hughes, and Kukiat Tudpor. 2022. "Tooth Loss, Cognitive Impairment and Fall Risk: A Cross-Sectional Study of Older Adults in Rural Thailand" International Journal of Environmental Research and Public Health 19, no. 23: 16015. https://doi.org/10.3390/ijerph192316015