
Moving Forward: Understanding Correlates of Physical Activity and Sedentary Behaviour during COVID-19 in Children and Adolescents—An Integrative Review and Socioecological Approach

 , , , , and
on behalf of the Welsh Institute of Physical Activity, Health, and Sport (WIPAHS)
, , , , and
on behalf of the Welsh Institute of Physical Activity, Health, and Sport (WIPAHS)
Abstract
:1. Introduction
2. Materials and Methods
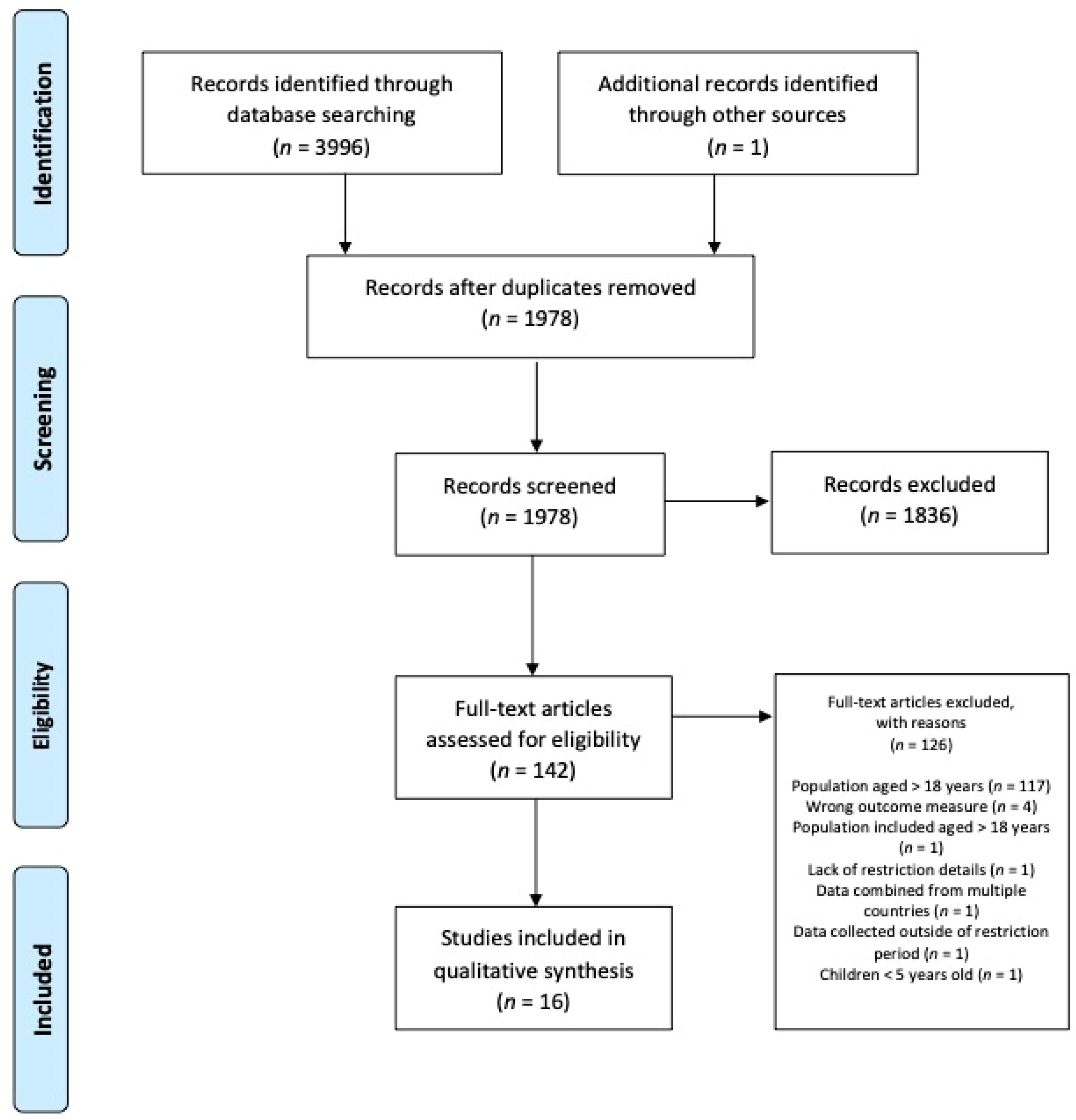
2.1. Literature Review Method
2.2. Quality Assessment
2.3. Data Analysis and Model Development
3. Results
3.1. Individual—Biological Factors
Age and Sex
3.2. Individual—Psychological Factors
3.2.1. Mental Health
3.2.2. Cognition, Motivation and Behaviour
3.3. Social Level Factors
3.3.1. Family Factors
3.3.2. Structured Support
3.4. Environmental Factors
Area of Residence and Resources
3.5. Policy Level Factors
COVID-19-Related Rules
4. Discussion
4.1. The COM-B: Behavioural Targets and Policy Recommendations
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1.6 million participants. Lancet Child Adolesc. Health 2019, 4, 23–35. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour. Available online: https://www.who.int/publications/i/item/9789240015128 (accessed on 11 August 2021).
- Rhodes, R.E.; Janssen, I.; Bredin, S.S.D.; Warburton, D.E.R.; Bauman, A. Physical activity: Health impact, prevalence, correlates and interventions. Psychol. Health 2017, 32, 942–975. [Google Scholar] [CrossRef]
- van Ekris, E.; Wijndaele, K.; Altenburg, T.M.; Atkin, A.J.; Twisk, J.; Andersen, L.B.; Janz, K.F.; Froberg, K.; Northstone, K.; Page, A.S.; et al. Tracking of total sedentary time and sedentary patterns in youth: A pooled analysis using the International Children’s Accelerometry Database (ICAD). Int. J. Behav. Nutr. Phys. Act. 2020, 17, 65. [Google Scholar] [CrossRef]
- Hamer, M.; Kivimäki, M.; Gale, C.R.; Batty, G.D. Lifestyle risk factors, inflammatory mechanisms, and COVID-19 hospitalization: A community-based cohort study of 387,109 adults in UK. Brain Behav. Immun. 2020, 87, 184–187. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Critical Preparedness, Readiness and Response Actions for COVID-19. Available online: https://apps.who.int/iris/handle/10665/336373 (accessed on 11 August 2021).
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef] [PubMed]
- Sedentary Behaviour Research, N. Letter to the editor: Standardized use of the terms “sedentary” and “sedentary behaviours”. Appl. Physiol. Nutr. Metab. 2012, 37, 540–542. [Google Scholar] [CrossRef] [Green Version]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too much sitting: The population health science of sedentary behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Cervero, R.B.; Ascher, W.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- van Kasteren, Y.F.; Lewis, L.K.; Maeder, A. Office-based physical activity: Mapping a social ecological model approach against COM-B. BMC Public Health 2020, 20, 163. [Google Scholar] [CrossRef]
- Toronto, C.E.; Remington, R. A Step-by-Step Guide to Conducting an Integrative Review, 1st ed.; Springer International Publishing: Cham, Swizterland, 2020; ISBN 978-3-030-37503-4. [Google Scholar]
- Knight, R.L.; McNarry, M.A.; Sheeran, L.; Runacres, A.W.; Thatcher, R.; Shelley, J.; Mackintosh, K.A. on behalf of the Welsh Institute of Physical Activity, Health, and Sport (WIPAHS). Moving forward: Understanding correlates of physical activity and sedentary behaviour during COVID-19—An integrative review and socioecological approach. Int. J. Environ. Res. Public Health 2021, 18, 10910. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Cochrane: Chichester, UK, 2021; Available online: https://training.cochrane.org/handbook/current (accessed on 28 February 2021).
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT), Version 2018; Registration of Copyright (#1148552); Canadian Intellectual Property Office, Industry Canada: Gatineau, QC, Canada, 2018. [Google Scholar]
- Hong, Q.N. Reporting the Results of the MMAT. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/140056890/Reporting%20the%20results%20of%20the%20MMAT.pdf (accessed on 9 February 2021).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Smith, B.; McGannon, K.R. Developing rigor in qualitative research: Problems and opportunities within sport and exercise psychology. Int. Rev. Sport Exerc. Psychol. 2018, 11, 101–121. [Google Scholar] [CrossRef]
- Dunton, G.F.; Do, B.; Wang, S.D. Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in children living in the U.S. BMC Public Health 2020, 20, 1351. [Google Scholar] [CrossRef] [PubMed]
- Ellis, W.; Dumas, T.M.; Forbes, L.M. Physically isolated but socially connected: Psychological adjustment and stress among adolescents during the initial COVID-19 crisis. Can. J. Behav. Sci. 2020, 52, 177–187. [Google Scholar] [CrossRef]
- Gilic, B.; Ostojic, L.; Corluka, M.; Volaric, T.; Sekulic, D. Contextualizing parental/familial influence on physical activity in adolescents before and during COVID-19 pandemic: A prospective analysis. Children 2020, 7, 125. [Google Scholar] [CrossRef]
- Guerrero, M.D.; Vanderloo, L.M.; Rhodes, R.E.; Faulkner, G.; Moore, S.A.; Tremblay, M.S. Canadian children’s and youth’s adherence to the 24-h movement guidelines during the COVID-19 pandemic: A decision tree analysis. J. Sport Health Sci. 2020, 9, 313–332. [Google Scholar] [CrossRef] [PubMed]
- McCormack, G.R.; Doyle-Baker, P.K.; Petersen, J.A.; Ghoneim, D. Parent anxiety and perceptions of their child’s physical activity and sedentary behaviour during the COVID-19 pandemic in Canada. Prev. Med. Rep. 2020, 20, 101275. [Google Scholar] [CrossRef]
- Medrano, M.; Cadenas-Sanchez, C.; Oses, M.; Arenaza, L.; Amasene, M.; Labayen, I. Changes in lifestyle behaviours during the COVID-19 confinement in Spanish children: A longitudinal analysis from the MUGI project. Pediatr. Obes. 2021, 16, e1273. [Google Scholar] [CrossRef]
- Mitra, R.; Moore, S.A.; Gillespie, M.; Faulkner, G.; Vanderloo, L.M.; Chulak-Bozzer, T.; Rhodes, R.E.; Brussoni, M.; Tremblay, M.S. Healthy movement behaviours in children and youth during the COVID-19 pandemic: Exploring the role of the neighbourhood environment. Health Place 2020, 65, 102418. [Google Scholar] [CrossRef]
- Moore, S.A.; Faulkner, G.; Rhodes, R.E.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.J.; Mitra, R.; O’Reilly, N.; Spence, J.C.; Vanderloo, L.M.; et al. Impact of the COVID-19 virus outbreak on movement and play behaviours of Canadian children and youth: A national survey. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 85. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.; Cooper, J.; McHale, F.; Clifford, J.; Woods, C. Barriers and facilitators to changes in adolescent physical activity during COVID-19. BMJ Open Sport Exerc. Med. 2020, 6, e000919. [Google Scholar] [CrossRef] [PubMed]
- Ozturk Eyimaya, A.; Yalçin Irmak, A. Relationship between parenting practices and children’s screen time during the COVID-19 pandemic in Turkey. J. Pediatr. Nurs. 2021, 56, 24–29. [Google Scholar] [CrossRef]
- Pombo, A.; Luz, C.; Rodrigues, L.P.; Ferreira, C.; Cordovil. R. Correlates of children’s physical activity during the COVID-19 confinement in Portugal. Public Health 2020, 189, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Sá, C.; Pombo, A.; Luz, C.; Rodrigues, L.P.; Cordovil, R. COVID-19 social isolation in Brazil: Effects on the physical activity routine of families with children. Rev. Paul. Pediatr 2020, 39, e2020159. [Google Scholar] [CrossRef] [PubMed]
- Sekulic, D.; Blazevic, M.; Gilic, B.; Kvesic, I.; Zenic, N. Prospective analysis of levels and correlates of physical activity during COVID-19 pandemic and imposed rules of social distancing; Gender specific study among adolescents from Southern Croatia. Sustainability 2020, 12, 4072. [Google Scholar] [CrossRef]
- Siegle, C.B.H.; Pombo, A.; Luz, C.; Rodrigues, L.P.; Cordovil, R.; Sá, C. Influences of family and household characteristics on children’s level of physical activity during social distancing due to COVID-19 in Brazil. Rev. Paul Pediatr. 2020, 39, e2020297. [Google Scholar] [CrossRef] [PubMed]
- Zenic, N.; Taiar, R.; Gilic, B.; Blazevic, M.; Maric, D.; Pojskic, H.; Sekulic, D. Levels and changes of physical activity in adolescents during the COVID-19 pandemic: Contextualizing urban vs. rural living environment. Appl. Sci. 2020, 10, 3997. [Google Scholar] [CrossRef]
- Zhang, X.; Zhu, W.; Kang, S.; Qiu, L.; Lu, Z.; Sun, Y. Association between physical activity and mood states of children and adolescents in social isolation during the COVID-19 epidemic. Int. J. Environ. Res. Public Health 2020, 17, 7666. [Google Scholar] [CrossRef]
- Kohrt, W.M.; Bloomfield, S.A.; Little, K.D.; Nelson, M.E.; Yingling, V.R. American College of Sports Medicine Position Stand: Physical activity and bone health. Med. Sci. Sports Exerc. 2004, 36, 1985–1996. [Google Scholar] [CrossRef] [Green Version]
- Okasha, M.; McCarron, P.; Gunnell, D.; Smith, G.D. Exposures in childhood, adolescence and early adulthood and breast cancer risk: A systematic review of the literature. Breast Cancer Res. Treat. 2003, 78, 223–276. [Google Scholar] [CrossRef] [PubMed]
- Liese, A.D.; Ma, X.; Maahs, D.M.; Trilk, J.L. Physical activity, sedentary behaviors, physical fitness, and their relation to health outcomes in youth with type 1 and type 2 diabetes: A review of the epidemiologic literature. J. Sport Health Sci. 2013, 2, 21–38. [Google Scholar] [CrossRef] [Green Version]
- Runacres, A.; Mackintosh, K.A.; Knight, R.L.; Sheeran, L.; Thatcher, R.; Shelley, J.; McNarry, M.A. Impact of the COVID-19 pandemic on sedentary time and behaviour in children and adults: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 11286. [Google Scholar] [CrossRef] [PubMed]
- Farooq, A.; Martin, A.; Janssen, X.; Wilson, M.G.; Gibson, A.M.; Hughes, A.; Reilly, J.J. Longitudinal changes in moderate-to-vigorous-intensity physical activity in children and adolescents: A systematic review and meta-analysis. Obes. Rev. 2020, 21, e12953. [Google Scholar] [CrossRef] [Green Version]
- Tudor-Locke, C.; Lee, S.M.; Morgan, C.F.; Beighle, A.; Pangrazi, R.P. Children’s pedometer-determined physical activity during the segmented school day. Med. Sci. Sports Exerc. 2006, 38, 1732–1738. [Google Scholar] [CrossRef]
- Eyler, A.; Nanney, M.S.; Brownson, R.C.; Lohman, D.; Haire-Joshu, D. Correlates of after-school activity preference in children ages 5–12. Am. J. Health Educ. 2006, 37, 69–77. [Google Scholar] [CrossRef]
- McGall, S.E.; McGuigan, M.R.; Nottle, C. Contribution of free play towards physical activity guidelines for New Zealand primary school children aged 7-9 years. Br. J. Sports Med. 2011, 45, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Hasson, R.; Sallis, J.F.; Coleman, N.; Kaushal, N.; Nocera, V.G.; Keith, N. COVID-19: Implications for physical activity, health disparities, and health equity. Am. J. Lifestyle Med. 2021. [Google Scholar] [CrossRef]
- Timo, J.; Sami, Y.P.; Anthony, W.; Jarmo, L. Perceived physical competence towards physical activity, and motivation and enjoyment in physical education as longitudinal predictors of adolescents’ self-reported physical activity. J. Sci. Med. Sport 2016, 19, 750–754. [Google Scholar] [CrossRef]
- Borhani, M.; Sadeghi, R.; Shojaeizadeh, D.; Harandi, T.F.; Vakili, M.A. Teenage girls’ experience of the determinants of physical activity promotion: A theory-based qualitative content analysis. Electron. Physician 2017, 9, 5075–5082. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Motion for Your Mind: Physical Activity for Mental Health Promotion, Protection and Care. Available online: https://www.euro.who.int/__data/assets/pdf_file/0018/403182/WHO-Motion-for-your-mind-ENG.pdf (accessed on 10 April 2021).
- Caputo, E.L.; Reichert, F.F. Studies of Physical Activity and COVID-19 during the Pandemic: A Scoping Review. J. Phys. Act. Health 2020, 17, 1275–1284. [Google Scholar] [CrossRef] [PubMed]
- Biddle, S.J.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhodes, R.E.; Lim, C. Promoting parent and child physical activity together: Elicitation of potential intervention targets and preferences. Health Educ. Behav. 2018, 45, 112–123. [Google Scholar] [CrossRef]
- Wiseman, N.; Harris, N.; Downes, M. Preschool children’s preferences for sedentary activity relates to parent’s restrictive rules around active outdoor play. BMC Public Health 2019, 19, 946. [Google Scholar] [CrossRef] [Green Version]
- Wang, G.; Zhang, Y.; Zhao, J.; Zhang, J.; Jiang, F. Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet 2020, 395, 945–947. [Google Scholar] [CrossRef]
- Biddle, S.J.; Gorely, T.; Pearson, N.; Bull, F.C. An assessment of self-reported physical activity instruments in young people for population surveillance: Project ALPHA. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population or participants and condition or interest | Children and adolescents aged 5–17 years Any sex/gender Not restricted to the UK | Studies including children aged <5 years (where separation of data was not possible) Studies including adults aged ≥ 18 years (where separation of data was not possible) |
| Intervention or exposures | Exposure to the COVID-19 pandemic, containment, and mitigation strategies | Studies that involve non-COVID-19 related pandemics, such as SARS or MERS |
| Comparison or control groups | No restrictions | |
| Outcomes of interest | Data/information, qualitative or quantitative, relating to correlates of PA and/or sedentary time/behaviour during the COVID-19 pandemic | No data relating to the pandemic phase or restrictions in place available Studies only including empirical data on volume of or changes in volume of PA or sedentary time/behaviour Data pooled from multiple different countries (where separation of data was not possible) |
| Setting | Any community setting | |
| Study designs | Any randomized, non-randomized, qualitative, or mixed methods study design providing original results | Studies not providing original results, such as systematic reviews, meta-analysis, general reviews, or editorials |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knight, R.L.; McNarry, M.A.; Runacres, A.W.; Shelley, J.; Sheeran, L.; Mackintosh, K.A., on behalf of the Welsh Institute of Physical Activity, Health, and Sport (WIPAHS). Moving Forward: Understanding Correlates of Physical Activity and Sedentary Behaviour during COVID-19 in Children and Adolescents—An Integrative Review and Socioecological Approach. Int. J. Environ. Res. Public Health 2022, 19, 1044. https://doi.org/10.3390/ijerph19031044
Knight RL, McNarry MA, Runacres AW, Shelley J, Sheeran L, Mackintosh KA on behalf of the Welsh Institute of Physical Activity, Health, and Sport (WIPAHS). Moving Forward: Understanding Correlates of Physical Activity and Sedentary Behaviour during COVID-19 in Children and Adolescents—An Integrative Review and Socioecological Approach. International Journal of Environmental Research and Public Health. 2022; 19(3):1044. https://doi.org/10.3390/ijerph19031044
Chicago/Turabian StyleKnight, Rachel L., Melitta A. McNarry, Adam W. Runacres, James Shelley, Liba Sheeran, and Kelly A. Mackintosh on behalf of the Welsh Institute of Physical Activity, Health, and Sport (WIPAHS). 2022. "Moving Forward: Understanding Correlates of Physical Activity and Sedentary Behaviour during COVID-19 in Children and Adolescents—An Integrative Review and Socioecological Approach" International Journal of Environmental Research and Public Health 19, no. 3: 1044. https://doi.org/10.3390/ijerph19031044