
Misuse of Anticholinergic Medications: A Systematic Review

 , , , , ,
, , , , ,  , ,
, ,  ,
,
Abstract
:1. Introduction
1.1. Abiuse of Medications
1.2. Abuse of Anticholinergic Medications
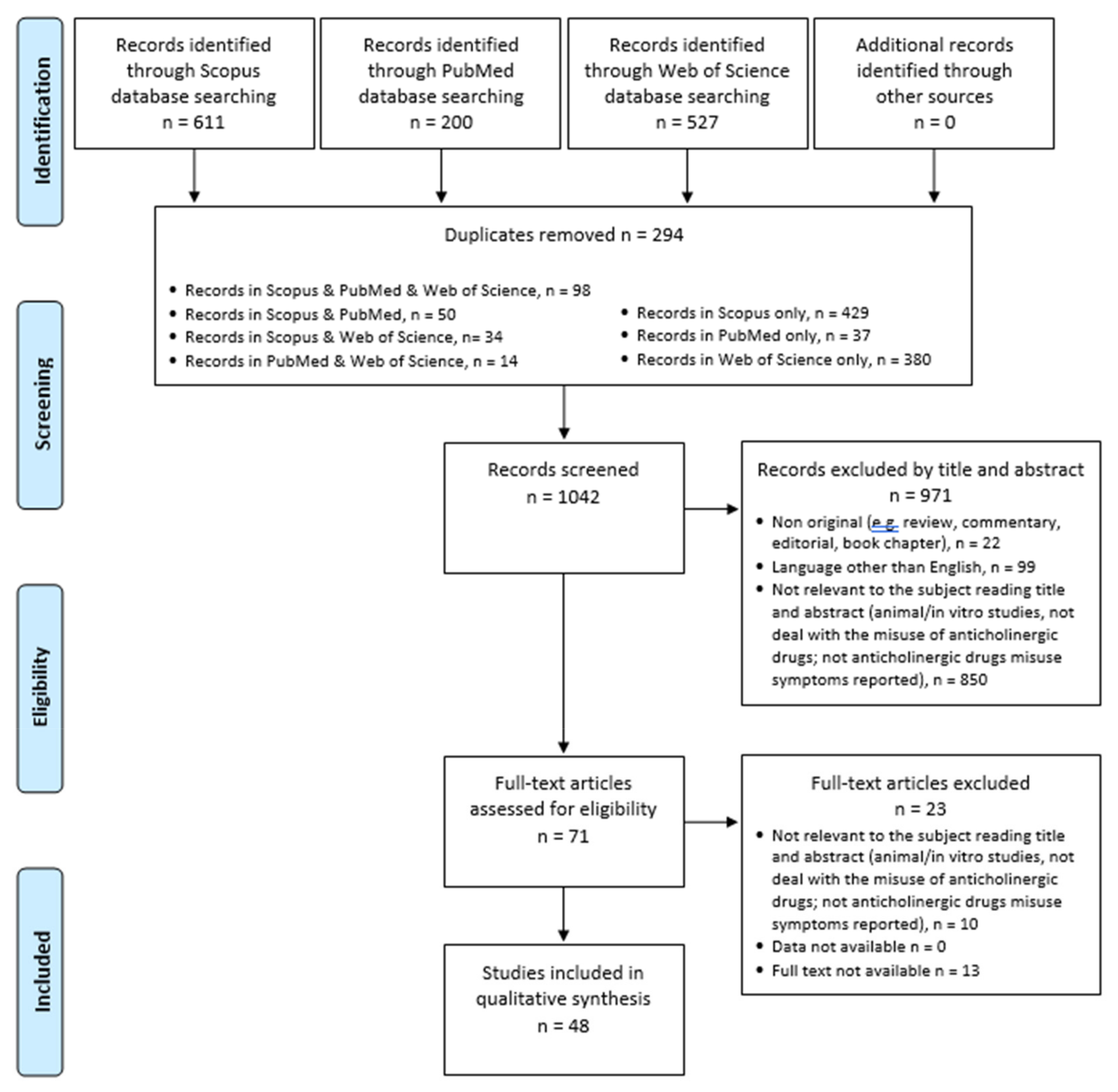
2. Materials and Methods
2.1. Systematic Review Procedures
2.2. Data Synthesis Strategy
3. Results
3.1. Benzhexol/Trihexyphenidyl (THP)
3.2. Benztropine
3.3. Atropine
3.4. Scopolamine/Scopolamine N-Butylbromide
3.5. Biperiden
3.6. Dicyclomine
3.7. Orphenadrine
3.8. Tropicamide
3.9. Glycopyrronium Tosylate
3.10. Oxybutynin
3.11. Pentolate, Prisoline, and Naphcon-A (Ophthalmic Drug)
3.12. Procyclidine
3.13. Unspecified Anticholinergic Drugs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chiappini, S.; Guirguis, A.; Corkery, J.M.; Schifano, F. Misuse of prescription and over-the-counter drugs to obtain illicit highs: How pharmacists can prevent abuse. Pharm. J. 2020, 305, 1–31. [Google Scholar]
- European Monitoring Centre for Drugs and Drug Addiction. Non-Medical Use of Medicines: Health and Social Responses [Internet]. 2021. Available online: https://www.emcdda.europa.eu/publications/mini-guides/non-medical-use-of-medicines-health-and-social-responses_en (accessed on 24 December 2021).
- Caplan, J.P.; Epstein, L.A.; Quinn, D.K.; Stevens, J.R.; Stern, T.A. Neuropsychiatric effects of prescription drug abuse. Neuropsychol. Rev. 2007, 17, 363–380. [Google Scholar] [CrossRef] [PubMed]
- Buhrich, N.; Weller, A.; Kevans, P. Misuse of anticholinergic drugs by people with serious mental illness. Psychiatr. Serv. 2000, 51, 928–929. [Google Scholar] [CrossRef]
- Zemishlany, Z.; Aizenberg, D.; Weiner, Z.; Weizman, A. Trihexyphenidyl (Artane) abuse in schizophrenic patients. Int. Clin. Psychopharmacol. 1996, 11, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Gjerden, P.; Bramness, J.G.; Slørdal, L. The use and potential abuse of anticholinergic antiparkinson drugs in Norway: A pharmacoepidemiological study. Br. J. Clin. Pharmacol. 2009, 67, 228–233. [Google Scholar] [CrossRef] [Green Version]
- Pullen, G.P.; Best, N.R.; Maguire, J. Anticholinergic abuse: A common problem? Br. Med. J. 1984, 289, 612–613. [Google Scholar] [CrossRef] [Green Version]
- Christensen, R.C. Screening for anticholinergic abuse in patients with chronic mental illness. Am. J. Emerg. Med. 2003, 21, 508. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Bernardo, W.M. PRISMA Statement and PROSPERO. Int. Braz. J. Urol. 2017, 43, 383–384. Available online: http://www.intbrazjurol.com.br/pdf/vol43n01/vol43n01_2017.pdf (accessed on 24 December 2021). [CrossRef] [Green Version]
- Goggin, D.A.; Solomon, G.F. Trihexyphenidyl abuse for euphorigenic effect. Am. J. Psychiatry 1979, 36, 459–460. [Google Scholar] [CrossRef]
- Harrison, G. The abuse of anticholinergic drugs in adolescents. Br. J. Psychiatry 1980, 137, 495. [Google Scholar] [CrossRef] [PubMed]
- Mohandas, E.; Kothari, V.C.; Vanvaria, S.K.; Mambwe, C.C.; Haworth, A. Trihexyphenidyl abuse. East Afr. Med. J. 1987, 64, 156–157. [Google Scholar] [PubMed]
- Deutsch, A.; Eyma, J. Massive ingestion of Trihexyphenidyl. Am. J. Psychiatry 1992, 149, 574–575. [Google Scholar] [PubMed]
- Kajimura, N.; Mizuki, Y.; Kai, S.; Suetsugi, M.; Yamada, M.; Okuma, T. Memory and cognitive impairments in a case of long-term trihexyphenidyl abuse. Pharmacopsychiatry 1993, 26, 59–62. [Google Scholar] [CrossRef]
- Kaminer, Y.; Munitz, H.; Wijsenbeek, H. Trihexyphenidyl (artane) abuse: Euphoriant and anxiolytic. Br. J. Psychiatry 1982, 140, 473–474. [Google Scholar] [CrossRef] [Green Version]
- Keshavan, M.S.; Burton, S.; Murphy, M.; Checkley, S.A.; Crammer, J.L. Benzexhol withdrawal and Cholinergic Mechanisms in Depression. Br. J. Psychiatry 1985, 147, 560–564. [Google Scholar] [CrossRef]
- Lo, Y.; Tsai, S.J. Trihexyphenidyl abuse in schizophrenic patient: A case report. Chin. Med. J. 1996, 57, 157–160. [Google Scholar]
- Macvicar, K. Abuse of antiparkinsonian drugs by psychiatric patients. Am. J. Psychiatry 1977, 134, 809–811. [Google Scholar]
- Petković, S.; Durendić-Brenesel, M.; Dolai, M.; Samojlik, I. Fatal Intoxication Because of Trihexyphenidyl. J. Forensic. Sci. 2011, 56, 1383–1386. [Google Scholar] [CrossRef]
- Rao, M.G.; Varambally, S.; Raveendranathan, D.; Venkatasubramanian, G.; Gangadhar, B.N. Trihexyphenidyl use and dependence: A case report. Ment. Health Subst. Use 2014, 7, 258–262. [Google Scholar] [CrossRef]
- Sofair, J.; Campion, J.; Angrist, B. High dose trihexyphenidyl abuse with psychological dependence. J. Clin. Psychopharmacol. 1983, 3, 263–264. [Google Scholar] [CrossRef]
- Fisch, R.Z. Trihexyphenidyl abuse: Therapeutic implications for negative symptoms of schizophrenia? Acta Psychiatr. Scand. 1987, 75, 91–94. [Google Scholar] [CrossRef] [PubMed]
- McInnis, M.; Petursson, H. Trihexyphenidyl dependence. Acta Psychiatr. Scand. 1984, 69, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Michael, A.; Murali, T.; Mathai, P.J.; Gopinath, P.S. Trihexylphenidyl dependence—Report of two cases. Indian J. Psychiatry 1984, 26, 178–179. [Google Scholar] [PubMed]
- Thunyapipat, C.; Manaboriboon, B.; In-iw, S.; Kriengsoontornkij, W. A Case Series of Trihexyphenidyl Abuse for Recreational Purpose in Thai Children and Adolescents. J. Adolesc. Health 2018, 62, S137. [Google Scholar] [CrossRef]
- Rubinstein, J.S. Antiparkinsonian drug abuse: Eight case reports. Hosp. Community Psychiatry 1979, 30, 34–37. [Google Scholar] [CrossRef]
- Mahal, P.; Nishanth, K.N.; Mahapatra, A.; Sarkar, S.; Balhara, Y.P.S. Trihexyphenidyl Misuse in Delusional Disorder. J. Neurosci. Rural Pract. 2018, 9, 428–430. [Google Scholar] [CrossRef]
- Younis, A.A.; Moselhy, H.F. Benzhexol-Dependence resulting from self-medication for intermittent explosive disorder. Int. J. Psychiatry Clin. Pract. 2009, 13, 11–15. [Google Scholar] [CrossRef]
- Crawshaw, J.A.; Mullen, P.E. A study of benzhexol abuse. Br. J. Psychiatry 1984, 145, 300–303. [Google Scholar] [CrossRef]
- Qureshi, N.A. Trihexyphenidyl (Artane) Abuse among Saudi Psychiatric Patients. Ann. Saudi Med. 1992, 12, 391–394. [Google Scholar]
- Qureshi, N.A.; Abdelgadir, M.H.; El-haraka, E.A. Trihexyphenidyl (Artane) Dependence: A Controlled. Ann. Saudi Med. 1997, 17, 185–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torrents, R.; Ferré, J.F.; Konareff, A.; Hemery, P.; Sherwin, K.; Lassalle, C.; Nicolas, S.; Sami, S. Misuse of Trihexyphenidyl (Artane) on Réunion Island. J. Clin. Psychopharmacol. 2018, 38, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Nappo, S.A.; De Oliveira, L.G.; Van Der Meer Sanchez, Z.; De Araújo Carlini, E. Trihexyphenidyl (Artane®): A Brazilian study of its abuse. Subst. Use Misuse 2005, 40, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Craig, D.H.; Rosen, P. Abuse of antiparkinsonian drugs. Ann. Emerg. Med. 1981, 10, 98–100. [Google Scholar] [CrossRef]
- Esang, M.; Person, U.S.; Izekor, O.O.; Le, T.K.; Ahmadian, D. An Unlikely Case of Benztropine Misuse in an Elderly Schizophrenic. Cureus 2021, 13, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Isbister, G.K.; Oakley, P.; Whyte, I.; Dawson, A. Treatment of anticholinergic-induced ileus with neostigmine. Ann. Emerg. Med. 2001, 38, 689–693. [Google Scholar] [CrossRef]
- Taylor, C.L.; Taylor, S.F. Atropine Autoinjector Use as a Suicidal Gesture. J. Emerg. Med. 2008, 34, 397–400. [Google Scholar] [CrossRef]
- Wang, H.E. Street Drug Toxicity Resulting from Opiates Combined with Anticholinergics. Prehosp. Emerg. Care 2002, 6, 351–354. [Google Scholar] [CrossRef]
- Weiner, A.L.; Bayer, M.J.; McKay, C.A.; DeMeo, M.; Starr, E. Anticholinergic poisoning with adulterated intranasal cocaine. Am. J. Emerg. Med. 1998, 16, 517–520. [Google Scholar] [CrossRef]
- Jalali, F.; Afshari, R.; Babaei, A. Smoking crushed hyoscine/scopolamine tablets as drug abuse. Subst. Use Misuse 2014, 49, 793–797. [Google Scholar] [CrossRef] [PubMed]
- Kummer, S.; Rickert, A.; Daldrup, T.; Mayatepek, E. Abuse of the over-the-counter antispasmodic butylscopolamine for the home synthesis of psychoactive scopolamine. Eur. J. Pediatr. 2016, 175, 1019–1021. [Google Scholar] [CrossRef] [PubMed]
- Strano-Rossi, S.; Mestria, S.; Bolino, G.; Polacco, M.; Grassi, S.; Oliva, A. Scopolamine fatal outcome in an inmate after buscopan® smoking. Int. J. Legal Med. 2021, 135, 1455–1460. [Google Scholar] [CrossRef]
- Affaticati, A.; Lidia Gerra, M.; Amerio, A.; Inglese, M.; Antonioni, M.C.; Marchesi, C. The controversial case of biperiden from prescription drug to drug of abuse. J. Clin. Psychopharmacol. 2015, 35, 749–750. [Google Scholar] [CrossRef] [Green Version]
- Ozucelik, D.N.; Yucel, N.; Coskun, S.; Cobanoglu, M.; Kunt, M.M. Gluteal abscess following intramuscular injection of dissolved biperiden tablets. Int. J. Clin. Pract. 2007, 61, 1417–1418. [Google Scholar] [CrossRef] [PubMed]
- Sinha, S.K.; Diman, S.; Sidana, A. A rare case of dicyclomineand mefenamic acid fulfilling criteria of dependence syndrome. Indian J. Psychiatry 2020, 62, 740–741. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Mondal, S.; Datta, A.; Bandyopadhyay, S. A rare case of dicyclomine abuse. J. Young Pharm. 2013, 5, 106–107. [Google Scholar] [CrossRef] [Green Version]
- Nissen, T. Toxic psychosis due to self-administered antiparkinson drug overdosage: A case report. Nord. J. Psychiatry 1987, 41, 25–26. [Google Scholar] [CrossRef]
- Schifano, F.; Marra, R.; Magni, G. Orphenadrine abuse. South Med. J. 1988, 81, 546. [Google Scholar] [CrossRef]
- Bozkurt, M.; Karabulut, V.; Evren, C.; Seker, M.; Kan, H. Intravenous abuse of tropicamide in opioid use disorder: Presentation of 2 cases. Subst. Abus. 2015, 36, 170–173. [Google Scholar] [CrossRef]
- Spagnolo, P.A.; Badiani, A.; Nencini, P. Polydrug abuse by intravenous use of heroin and tropicamide-containing eyedrops. Clin. Neuropharmacol. 2013, 36, 100–101. [Google Scholar] [CrossRef] [PubMed]
- Michael, T.; Paul, C. A new medication, a new toxidrome—A case report of anticholinergic wipe toxicity due to improper medication use. Am. J. Emerg. Med. 2021, 46, 797.e1–797.e2. [Google Scholar] [CrossRef] [PubMed]
- Balasar, M.; Çiçekçi, F. Oxybutynin addiction amongst prisoners: Two case reports. Anadolu Psikiyatr. Derg. 2016, 17, 77–79. [Google Scholar] [CrossRef] [Green Version]
- Al-Khalaileh, W.; Abu-Farha, R.; Wazaify, M.; Van Hout, M.C. Ophthalmic drug abuse: An observational study from community pharmacies. Res. Soc. Adm. Pharm. 2019, 15, 943–948. [Google Scholar] [CrossRef]
- Coid, J.; Strang, J. Mania secondary to procyclidine abuse. Br. J. Psychiatry 1982, 141, 81–84. Available online: http://www.ncbi.nlm.nih.gov/pubmed/7116076 (accessed on 24 December 2021). [CrossRef]
- Wells, B.; Marken, P.; Rickman, L.; Brown, C.; Hamann, G.; Grimmig, J. Characterizing anticholinergic abuse in community mental health. J. Clin. Psychopharmacol. 1989, 9, 431–435. [Google Scholar] [CrossRef]
- Naja, W.J.; Halaby, A. Anticholinergic Use and Misuse in Psychiatry: A Comprehensive and Critical Review. J. Alcohol. Drug Depend. 2017, 5, 5–8. [Google Scholar] [CrossRef]
- Katzung, B.G.; Vanderah, T.W. Notice. In Basic & Clinical Pharmacology, 15th ed.; McGraw-Hill: New York, NY, USA, 2021; Available online: http://accesspharmacy.mhmedical.com/content.aspx?aid=1176460635 (accessed on 24 December 2021).
- Dose, M.; Tempel, H.D. Abuse potential of anticholinergics. Pharmacopsychiatry 2000, 33, 43–46. [Google Scholar] [CrossRef]
- Gerretsen, P.; Pollock, B.G. Drugs with anticholinergic properties: A current perspective on use and safety. Expert Opin. Drug Saf. 2011, 10, 751–765. [Google Scholar] [CrossRef]
- Martinotti, G.; De Risio, L.; Vannini, C.; Schifano, F.; Pettorruso, M.; Di Giannantonio, M. Substance-Related exogenous psychosis: A postmodern syndrome. CNS Spectr. 2021, 26, 84–91. [Google Scholar] [CrossRef]
- Rubinstein, J.S. Abuse of Antiparkinsonism Drugs: Feigning of Extrapyramidal Symptoms to Obtain Trihexyphenidyl. JAMA J. Am. Med. Assoc. 1978, 239, 2365–2366. [Google Scholar] [CrossRef] [PubMed]
- Marken, P.A.; Stuart Munro, J. Selecting a selective serotonin reuptake inhibitor: Clinically important distinguishing features. Prim. Care Companion J. Clin. Psychiatry 2000, 2, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Barrett, S.P.; Meisner, J.R.; Stewart, S.H. What constitutes prescription drug misuse? Problems and pitfalls of current conceptualizations. Curr. Drug Abuse Rev. 2008, 1, 255–262. [Google Scholar] [CrossRef]
- Casati, A.; Sedefov, R.; Pfeiffer-Gerschel, T. Misuse of medicines in the European union: A systematic review of the literature. Eur. Addict. Res. 2012, 18, 228–245. [Google Scholar] [CrossRef]
- Novak, S.P.; Håkansson, A.; Martinez-Raga, J.; Reimer, J.; Krotki, K.; Varughese, S. Nonmedical use of prescription drugs in the European Union. BMC Psychiatry 2016, 16, 274. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Ref (Name, Year) | Country | Study Design | Population | Mean Age (yrs) ± sd | Psychiatric Comorbidity | Medical Comorbidity | Route of Administration and Dosage | Physical Symptoms | Psychiatric Symptoms | Polyabuse | Outcome | Notes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ATROPINE | ||||||||||||
| Taylor et al., 2007 | North Carolina (USA) | Case report | N = 1; F | 29 | None | None | IM, 4 mg | Tachycardia, tachypnoea, dilatated pupils, dry mucous membranes, dry skin, urinary retention | Anxiety | 30 meloxicam tablets, alcohol | Activated charcoal with sorbitol, IV fluids | Symptoms resolved over a 6 h period of observation |
| Wang, 2002 | Pennsylvania (USA) | Case report | N = 1; F | 41 |
| None | Oral | Pupils dilated, dry skin, sinus bradycardia, ataxia. After IV naloxone: tachycardia, tachypnoea, hypertension | Slurred speech. After IV naloxone: agitation, delirium, disorientation | Codeine and morphine mixed with atropine | IV Naloxone, IV Lorazepam, rapid-sequence intubation, orogastric lavage, and activated charcoal | During hospitalization: persistent agitation refractory to benzodiazepine, pneumonia, and stress gastritis |
| Weiner et al., 1998 | Connecticut (USA) | Case report | N = 1; M | 39 |
| None | Nasal | Tachycardia, hypertension, warm and dry skin, facial flushing, dilated pupils minimally reactive to light, absence of bowel sounds | Agitation, intermittent delirium; disorientation | Cocaine | IV Lorazepam 1 mg, activated charcoal 50 g, cathartic mixture | Patient ingested cocaine adulterated with atropine |
| BENZHEXOL/TRIHEXYPHENIDYL (THP) | ||||||||||||
| Crawshaw et al., 1984 | New Zealand | Observational study | N = 21; M = 17 | 21 ± 6 |
| Extra-pyramidal side-effects of neuroleptic medication in patients with schizophrenia | Oral, 15–60 mg | Dehydration, tachycardia, pronounced thirst, and blurred vision | Toxic-confusional state with psychosis and visual hallucinations, illusions, and distorted time sense (N = 10); difficulties in recent memory and new learning were associated with problems of attention and concentration (N = 6) | Alcohol, cannabis (N = 12), hallucinogens (N = 10), opiates (N = 10), amphetamines (N = 9), benzodiazepines (N = 7), cough mixtures, solvents, cocaine, and various neuroleptics | NA | |
| Deutsch et al., 1992 | New York (USA) | Case report | N = 1; F | 33 |
| Cerebral palsy | Oral, maximum 105 mg (21 tablets) in a few hours in each time | Dry skin, dry mouth, and blurred vision | Restlessness, depression, confusion, disorientation, and auditory and visual hallucinations | None | IV lorazepam | Anticholinergic psychosis with hallucinosis |
| Fisch et al., 1987 | Israel | Case series | N = 14; M = 5 | 21–30 |
| None | Oral, 20–60 mg | None |
| Heroin, diazepam | NA | One patient feigned extrapyramidal symptoms in order to obtain THP |
| Goggins et al., 1979 | Norway | Case Report | N = 1; M | 40 |
| Weight loss | Oral 35–40 mg/die | Tachycardia and nausea | Restlessness, euphoria | None | NA | |
| Harrison, 1980 | England (UK) | Case Report | N = 1; M | 19 |
| NA | Oral | Swollen abdomen | Euphoria | NA | NA | |
| Kajimura et al., 1993 | Japan | Case report | N = 1; M | 55 | None | Essential tremor | Oral, 20 mg/day for 18 years | Headache, tachycardia, and general fatigue | Memory loss, cognitive impairment. On withdrawal: anxiety, irritability, insomnia, perspiration, and anorexia | None | After stopping THP, clotiazepam and flunitrazepam were used to manage withdrawal | |
| Kaminer et al., 1982 | Israel | Case report | N = 1; M | 30 |
| None | Oral, 30–40 mg/die | Dystonic reaction, withdrawal symptoms, and tachycardia | Acute: auditory hallucinations Chronic: anxiety reduction, sleep disturbance, and euphoria | Cannabis, LSD, amphetamines, barbiturates, and alcohol | Treated with haloperidol 10 mg | The patient used to mix drugs and THP |
| Keshavan et al., 1985 | England (UK) | Case report | N = 1; M | 38 |
| None | Oral, 70 mg | NA | Euphorigenic effect, auditory and visual hallucinations | Pimozide 8 mg, lorazepam 2,5 mg day | Admitted to psychiatric ward, gradually reduction of benzhexol with withdrawal symptoms, agitation, depression, and exacerbation of auditory hallucinations | |
| Lo et al., 1996 | Taiwan | Case report | N = 1; M | 35 |
| None | Oral, 200 mg/day for 2 years | None | Delusion of reference, thought broadcasting, loosening of association, paralogical thinking, auditory hallucination | None | Decreased dosage of THP and clonazepam | Patient feigned extrapyramidal syndrome to obtain biperiden injection |
| Macvicar, 1977 | California (USA) | Case report | N = 1; M | 30 |
| None | Oral 24–30 mg/die | Dry mouth and constipation | Toxic psychosis, hallucinations, euphoria, and talkativeness | NA | NA | |
| Mahal et al., 2018 | Delhi (India) | Case series | N = 2; M | 32 |
| 1st case: headache, recurrent abdominal pain; 2nd case: none | Oral, 40–60 mg | 1st case: headache, sweating, and tachycardia; 2nd case: none | Drug abuse aimed to obtain relaxation; withdrawal symptoms were restlessness, irritability, and aggressiveness | 1st case: nicotine and alprazolam; 2nd case: nicotine and opioid | NA | History of multiple prescription drug misuse |
| Mclnnis et al., 1984 | Iceland | Case series | N = 2; M = 1 | 25 and 35 |
| None | Oral, 40 mg | Ataxia, headache, visual difficulties, and photophobia | Confusion, self-harm, disorientation, agitation, bizarre behavior with difficulties of speech, and reduced concentration | Haloperidol, benzodiazepines, alcohol; perfenazine (100 mg IM every 2 weeks), chlorpromazine 50 mg, and clomipramine | NA | |
| Michael et al., 1984 | Karnataka (India) | Case series | N = 2; M | 28 and 30 |
| None | Oral, 6 mg | None | None | Trifluoperazine 15–20 mg, chlorpromazine 300–600 mg | Withdrawal symptoms including agitation, tachycardia, restlessness, aggressiveness, lethargy, giddiness, sweating, and craving | |
| Mohan et al., 1981 | Delhi (India) | Case report | N = 1; M | 35 |
| None | Oral 120–140 mg/die | NA | Visual hallucinations, paranoid ideas, and ideas of reference | NA | NA | |
| Nappo et al., 2005 | São Paulo (Brazil) | Survey | N = 37; M = 29 | 20–30 yy =14; 30–40 yy =18; >40 yy = 5 | None | NA | Oral, from one-half to four pills (3–8 mg) | Dry mouth, gastritis, vomiting, tachycardia, urinary retention, and dental caries | Euphoria, hallucinations, delirium, nervousness, aggressiveness, memory loss, decreased attention, loss of appetite, insomnia, and depression | Alcohol, coffee, nicotine | NA | THP was neither the initial drug in the substance user’s career nor their main drug |
| Petkovic et al., 2012 | Serbia | Case report | N = 1; F | 59 |
| None | Oral, 15 mg | NA | NA | None | Death | THP blood and urine concentrations were those associated with fatalities |
| Qureshi, 1992 | Saudi Arabia | Observational study | N = 14; M = 13 | 27.93 ± 6.55 |
| NA | Oral | Tardive dyskinesia, extrapyramidal symptoms | Symptoms of withdrawal included palpitations, restlessness, body aches, lethargy, irritability, aggression, discomfort, craving, and anxiety | Polydrug abuse (57.14%) | THP on a prophylactic basis with improvement in negative symptoms | |
| Qureshi et al., 1997 | Saudi Arabia | Case control | N = 30; M = 25 | 33.83 ± 7.4 |
| NA | Oral | Dyskinetic movements | Drug abusers were characterized by less negative symptoms | Some 53% abused beverages, amphetamines, and benzodiazepines | NA | |
| Rao et al., 2014 | Karnataka (India) | Case report | N = 1; F | 55 |
| None | Oral | NA | Increased speech output, psychomotor agitation, and reduced need for sleep | None | Treated with clonazepam, haloperidol 10 mg/day, and THP 4 mg/day | |
| Rubinstein, 1979 | California (USA) | Case series | N = 8 (N = 6 related to THP), 4 M, 2 F | 25–32 |
| None | Oral, 15–250 mg/die | Eye-rolling and finger stiffness | When recorded (cases 2–3), bizarre and violent behavior, difficulty in speech, and hallucinations were described; in some cases, high-dosage THP was taken to get high | Diazepam, LSD, amphetamines, thiothixene, cannabis, and PCP | Case 5 was treated with diazepam and fluphenazine for PCP-induced toxic psychosis | Most of the patients continued to ask for THP during the hospitalization |
| Sofair et al., 1983 | New York (USA) | Case report | N = 1; M | 24 |
| None | Oral, 60 mg/die | Dry mouth, constipation | Relaxation and impaired concentration | THP addiction | Abrupt cessation of THP | |
| Thunyapipat et al., 2018 | Thailand | Case series | N = 27, M = 15 | 14.2 (range 10.6–21) |
| NA | Oral, from 1 to 50 tablets once | No peripheral anticholinergic symptoms | Agitation, hallucination | Unspecified drug abuse (63.6%) | Motivational interviewing in 68.4% of hospitalized cases | Of those who received motivational interviewing, all discontinued abusing THP at a monthly follow-up visit |
| Torrents et al., 2018 | France | Cohort study | N = 69; M = 67, F = 2 | 36 |
| NA | Oral | NA | The abuse aimed to reach anxiolytic, sedative, and stimulating effects or to control the use of another drug; reported side effects were behavioral disorders such as aggressiveness, agitation, and paranoia | Tobacco (72%), benzodiazepines, cannabis, alcohol | Not reported | |
| Younis et al., 2009 | United Arab Emirates | Observational study | N = 190 | 29.5 (19–52) |
| NA | Oral | NA | The abuse aimed to relax and control aggressive outbursts | Alcohol, cannabis, cocaine, and opioids | 95 patients had difficulty stopping taking benzhexol | |
| Zemishlany et al., 1996 | Israel | Case control | N = 14; M = 11 | 34 ± 5.3 |
| NA | Oral, >20 mg | NA | Thinking disturbance, withdrawal retardation, hostile suspiciousness, anxious depression | Cannabis and alcohol | Neuroleptic treatment | |
| BENZTROPINE | ||||||||||||
| Craig et al., 1981 | Colorado (USA) | Case series | N = 2; M = 1 | 19 and 22 | NA | None | Oral, 120–140 mg | 1st case: dilated pupils, dry skin, urinary retention; 2nd case: tachycardia, fever, hypertension, dilatated pupils, warm and dry skin | 1st case: agitation, bizarre behavior, altered mental status; 2nd case: hallucinations, flight of ideas, agitation, combativeness | 1st case: abuse of sedative-hypnotics and oral narcotics; 2nd case: speed, LSD, alcohol | 1st case: treated with physostigmine, discharged 18 h later; 2nd case: treated with physostigmine | Diagnostic trial of physostigmine |
| Esang et al., 2021 | Pennsylvania (USA) | Case report | N = 1; M | 67 |
| Benign prostatic hyperplasia; essential hypertension | Oral | Hematochezia, abdominal pain, constipation, and difficulty with urination | None | None | Spontaneous remission of symptoms after returning to therapeutic doses | |
| Isbister et al., 2003 | Australia | Case report | N = 1; M | 33 |
| Hypertension; epilepsy; cluster headache | Oral, 27 tablets (2 mg each) during the previous 6 days | Abdominal pain, distention, drowsiness, hypertension, tachycardia, blurred vision, anticholinergic-induced ileus with absent bowel sound | Confusion, hallucinations, delirium | NA | IV fluids, meperidine, IV neostigmine 2 mg + 2.5 mg | |
| Rubinstein, 1979 | California (USA) | Case report | N = 8 (N = 2 were related to benztropine, M) | 26 and 28 | Schizophrenia | NA | Oral/IM | Stiffness and eye rolling | Nervousness | Drug abuse (heroin, alcohol, unspecified) | Treated with thioridazine and diazepam | |
| BIPERIDEN | ||||||||||||
| Affaticati et al., 2015 | Italy | Case report | N = 1; M | 27 | None | Withdrawal syndrome symptoms, e.g., headache | Oral 16 mg/die | Urinary retention | Mild confusional state with temporal, spatial disorientation, impairment of attention and concentration, psychomotor agitation | Trihexyphenidyl, cocaine, alcohol, cannabis | Biperiden gradually tapered; the patient was also treated with quetiapine, 50 mg/d | After 6 months, he stopped using biperiden |
| Ozucelik et al., 2007 | Turkey | Case report | N = 1; M | 52 |
| None | 120 mg IM (60 biperiden tablets) | Swelling and pain caused by an abscess in injection site. Mildly elevated hepatic function tests | NA | NA | General surgery for abscess drainage and antibiotics | |
| DICYCLOMINE | ||||||||||||
| Sinha et al., 2020 | Chandigarh (India) | Case report | N = 1; M | 30 | None | Dysmenorrhea, headache | Oral 10–15 tablets per day, 50–75 mg/day | Tachycardia, palpitation, sweating | Withdrawal symptoms, anxiety | Dicyclomine and mefenamic acid | Reversion to normal physiological state in a week after being treated with fluoxetine 20 mg per day and clonazepam 0.5 mg per day | |
| Das et al., 2013 | Bengal (India) | Case report | N = 1; F | 18 | None | None | IM | Weakness, palpitation, fever, blurred vision, sweating, dry skin | Confusion, withdrawal reaction, anxiety, depression, anorexia | None | Treated with IV physostigmine with remission in a week | Drug use began with drug treatment for enterocolitis |
| GLYCOPYRRONIUM TOSYLATE | ||||||||||||
| Tarr et al., 2021 | Bronx (USA) | Case report | N = 1; F | 14 |
| Acne vulgaris | Topical | Progressive myopia, dry mouth, anhidrosis, urinary hesitancy, and chronic constipation | None | None | Discharged at home after monitoring spontaneous remission | Patient would possibly have access to other medication when unsupervised |
| ORPHENADRINE | ||||||||||||
| Nissen et al., 1987 | Norway | Case report | N = 1; F | 26 |
| None | Oral, 800 mg | Dry and warm, pupils dilated, asymmetrical abdominal reflexes | Disorientation, clouding of consciousness, agitation, aggressivity, pressured speech and laughing with loosening of associations, psychosis with mystic-megalomanic delusion and visual hallucinations | Levodopa 2000 mg; benserazide chloride 400 mg; alcohol | Admitted to psychiatric ward | |
| Schifano et al., 1988 | Italy | Case report | N = 1; M | 24 |
| Not reported | Oral, up to 1250–1500 mg/day over a period of 2 months | Dizziness, tremor | Euphoria, visual hallucinations, mood enhancement, unpleasant misperceptions | NA | Drug stopped because difficult to obtain | Haloperidol and orphenadrine prescribed for hallucinations |
| OXYBUTYNIN | ||||||||||||
| Balasar et al., 2016 | Turkey | Case series | N = 2; M | 27 and 45 |
| overactive bladder | Oral, 100–150 mg/day and 300–400 mg/day | Xerostomia, constipation, urinary arrest | Relief from the need of using drugs and alcohol | None | NA | |
| PENTOLATE, PRISOLINE, AND NAPHCON-A (OPHTHALMIC DRUG) | ||||||||||||
| Al-Khalaileha et al., 2019 | Jordan | Observational study | N = 140; M:79; F: 51 | <20 yy: 13; 21–40 yy: 81; 41–50 yy: 29; 50–60 yy: 5; >60 yy: 2 | NA | NA | Topical | Conjunctivitis, eczematoid blepharoconjunctivitis, and conjunctival hyperemia | The abuse was aimed to relax, get high, induce pleasure, and boost energy | NA | NA | N = 19 cases have been suspected for abuse |
| PROCYCLIDINE | ||||||||||||
| Coid, 1982 | England (UK) | Case report | N = 1; M | 36 |
| None | Oral 40 mg | NA | Disinhibition, mania, aggressiveness | Physeptone® (methadone), alcohol | ||
| SCOPOLAMINE/SCOPOLAMINE N-BUTYLBROMIDE | ||||||||||||
| Jalali et al., 2014 | Iran | Cross-sectional case series | N = 36; M | 27–42 | None | None | Smoked tablets | Dry mouth, dry throat, bowel movement, palpitation, blurred vision, flushing | Insomnia, irritability, inability to concentrate, incoherent speech, slurred speech, amnesia, illogical thinking and hallucinations | Substance abuse (on methadone) | Not reported | |
| Kummer et al., 2015 | Germany | Case series | N = 2; M | 16 and 15 | None | None | Oral 40 mg una tantum | Flushed and dry skin, tachycardia | 1st case: severe agitation, disorientation, intermittent aggressive behavior, nonsensical speech; 2nd: partial amnesia | None | Transferred to intensive care unit, he was treated with midazolam and haloperidol; both were discharged from hospital 2 days later | |
| Strano-Rossi et al., 2021 | Italy | Case report | N = 1; M | 41 | SUD | Multiple traumas from aggression | Smoked tablets | Cerebral and lung edema | NA | Cannabis | Death | Other drugs identified in urine and blood included benzodiazepines, antipsychotic drugs in therapeutic or subtherapeutic concentrations |
| TROPICAMIDE | ||||||||||||
| Bozkurt et al., 2014 | Turkey | Case series | N = 2; 1 M; 1 F | 37–38 | None | None | IV | 1st case: decreased appetite, weight loss, and blurred vision; 2nd case: palpitations and sweating | 1st case: the patient experienced relief and relaxation mixing tropicamide and heroin; hallucinations and dissociation were recorded; 2nd case: dissociation, anxiety, and concentration problems | 1st case: cocaine, clonazepam, ecstasy, cannabis, and heroin; 2nd case: alprazolam, codeine, cocaine, and ecstasy | 1st case: treated with naloxone and opioid withdrawal symptoms; discharged after 14 days of hospitalization; 2nd case: discharged with quetiapine 100 mg/day treatment | Tropicamide was mixed with heroin |
| Spagnolo et al., 2013 | Italy | Case report | N = 1; F | 22 | None | None | IV | Palpitations, hypertension, tachycardia, fever, mydriasis, warm and flushed skin, and xerostomia | Euphoria, hallucinations | Heroin | Treated with diazepam | |
| UNSPECIFIED ANTICHOLINERGIC DRUGS | ||||||||||||
| Wells. et al., 1990 | Tennessee USA) | Controlled prospective study | N = 21; M = 14 | 33.6 ± 6.1 |
| NA | NA | Dehydrated skin, tachycardia, blurred vision, and thirst | Relaxation (N = 17), elevated mood (N = 15), energy (N = 14), reduced concentration (N = 11), visual hallucinations (N = 4), confusion (N = 3), and auditory hallucinations (N = 3) | Antipsychotics | NA | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiappini, S.; Mosca, A.; Miuli, A.; Semeraro, F.M.; Mancusi, G.; Santovito, M.C.; Di Carlo, F.; Pettorruso, M.; Guirguis, A.; Corkery, J.M.; et al. Misuse of Anticholinergic Medications: A Systematic Review. Biomedicines 2022, 10, 355. https://doi.org/10.3390/biomedicines10020355
Chiappini S, Mosca A, Miuli A, Semeraro FM, Mancusi G, Santovito MC, Di Carlo F, Pettorruso M, Guirguis A, Corkery JM, et al. Misuse of Anticholinergic Medications: A Systematic Review. Biomedicines. 2022; 10(2):355. https://doi.org/10.3390/biomedicines10020355
Chicago/Turabian StyleChiappini, Stefania, Alessio Mosca, Andrea Miuli, Francesco Maria Semeraro, Gianluca Mancusi, Maria Chiara Santovito, Francesco Di Carlo, Mauro Pettorruso, Amira Guirguis, John Martin Corkery, and et al. 2022. "Misuse of Anticholinergic Medications: A Systematic Review" Biomedicines 10, no. 2: 355. https://doi.org/10.3390/biomedicines10020355