Exploring the Baseline Knowledge and Experience of Healthcare Professionals in the United Kingdom on Novel Psychoactive Substances


 ,
,  , , and
, , and
Abstract
:1. Background
1.1. Current NPS Drug Scenes, Related Implications and Responses within the Healthcare System
1.2. Studies Exploring NPS Knowledge Among Healthcare Professionals (HCPs)
2. Methods
2.1. Survey Design
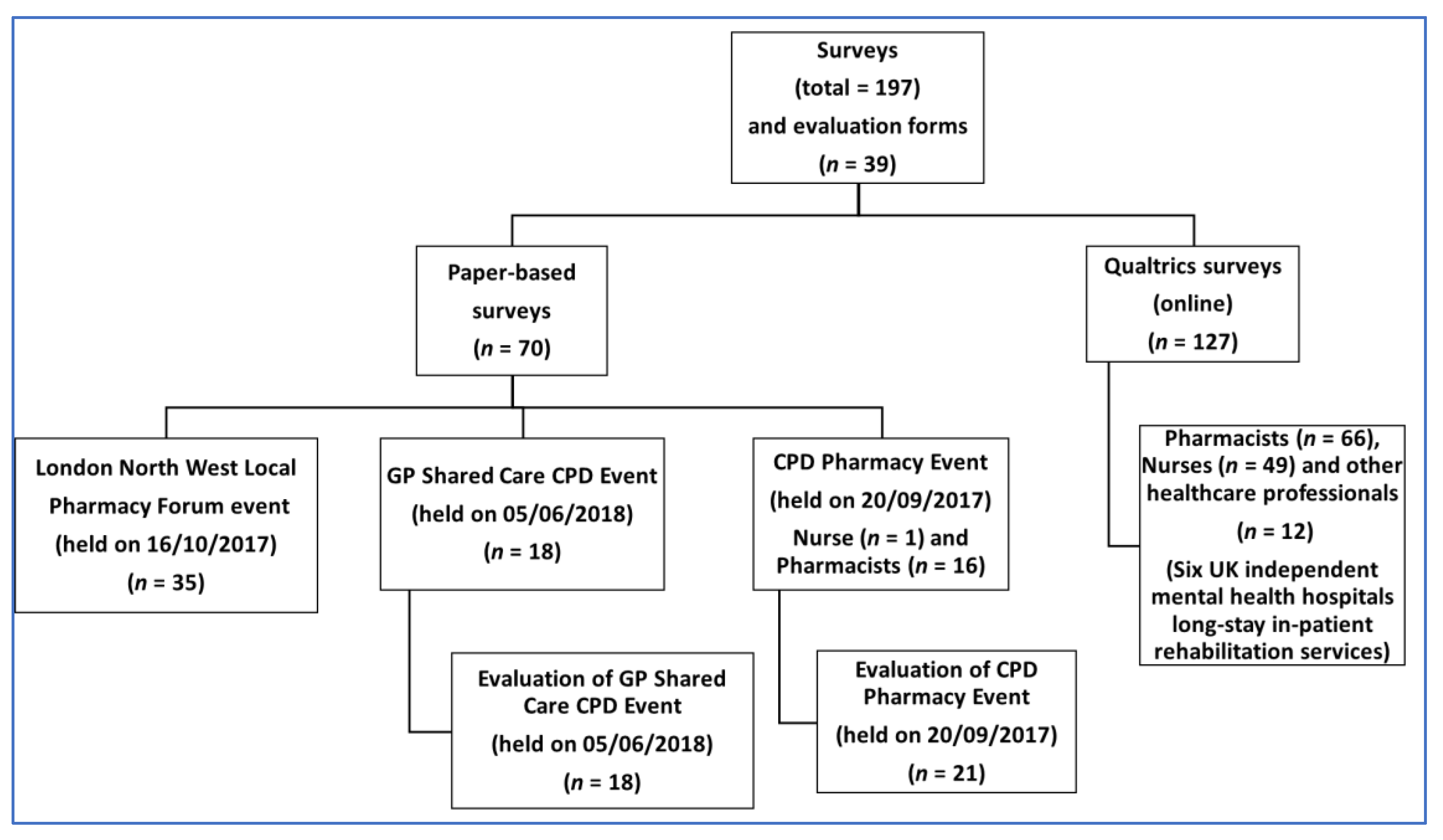
2.2. Survey Distribution
2.3. Data Extraction, Cleaning and Analysis
3. Results
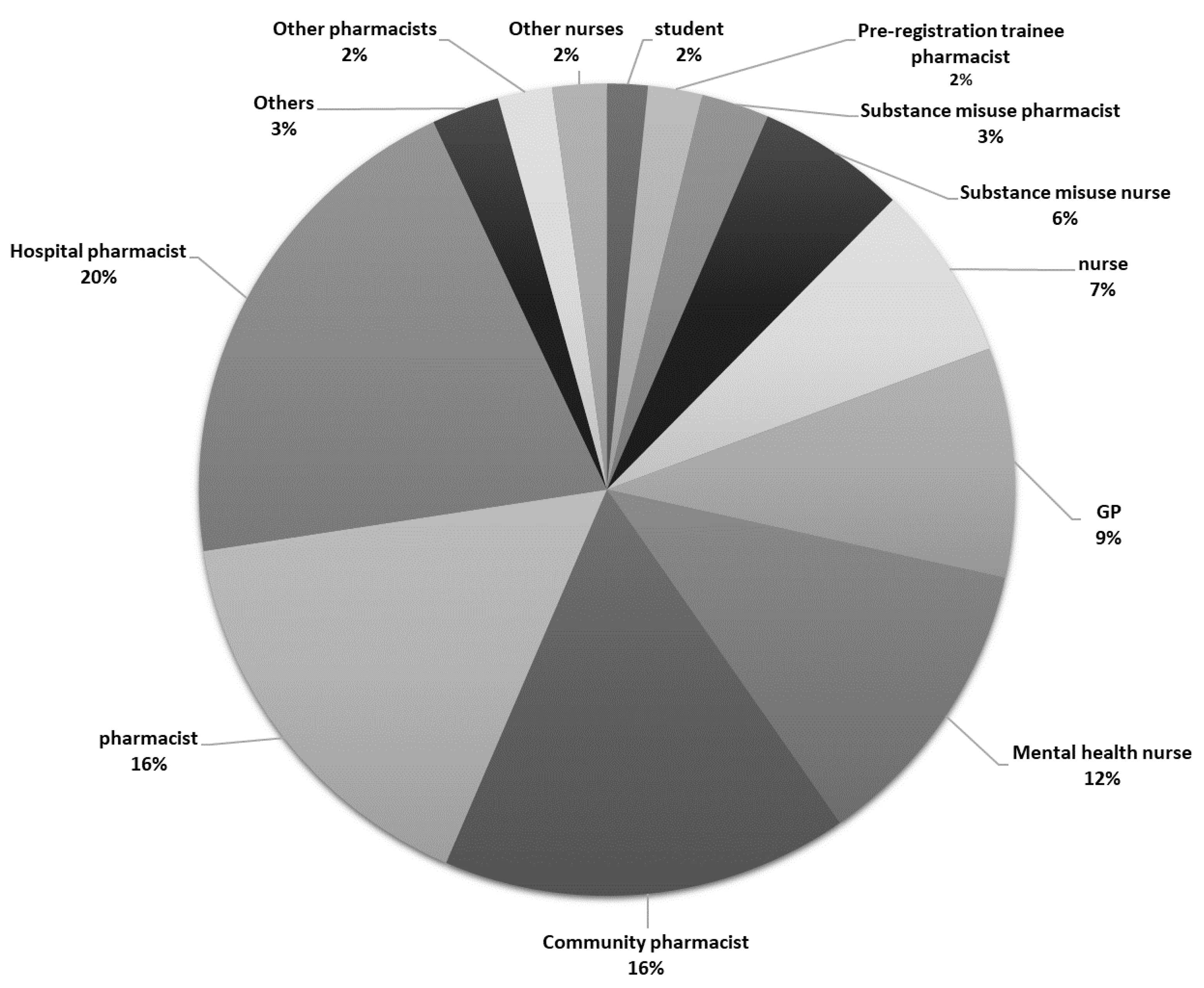
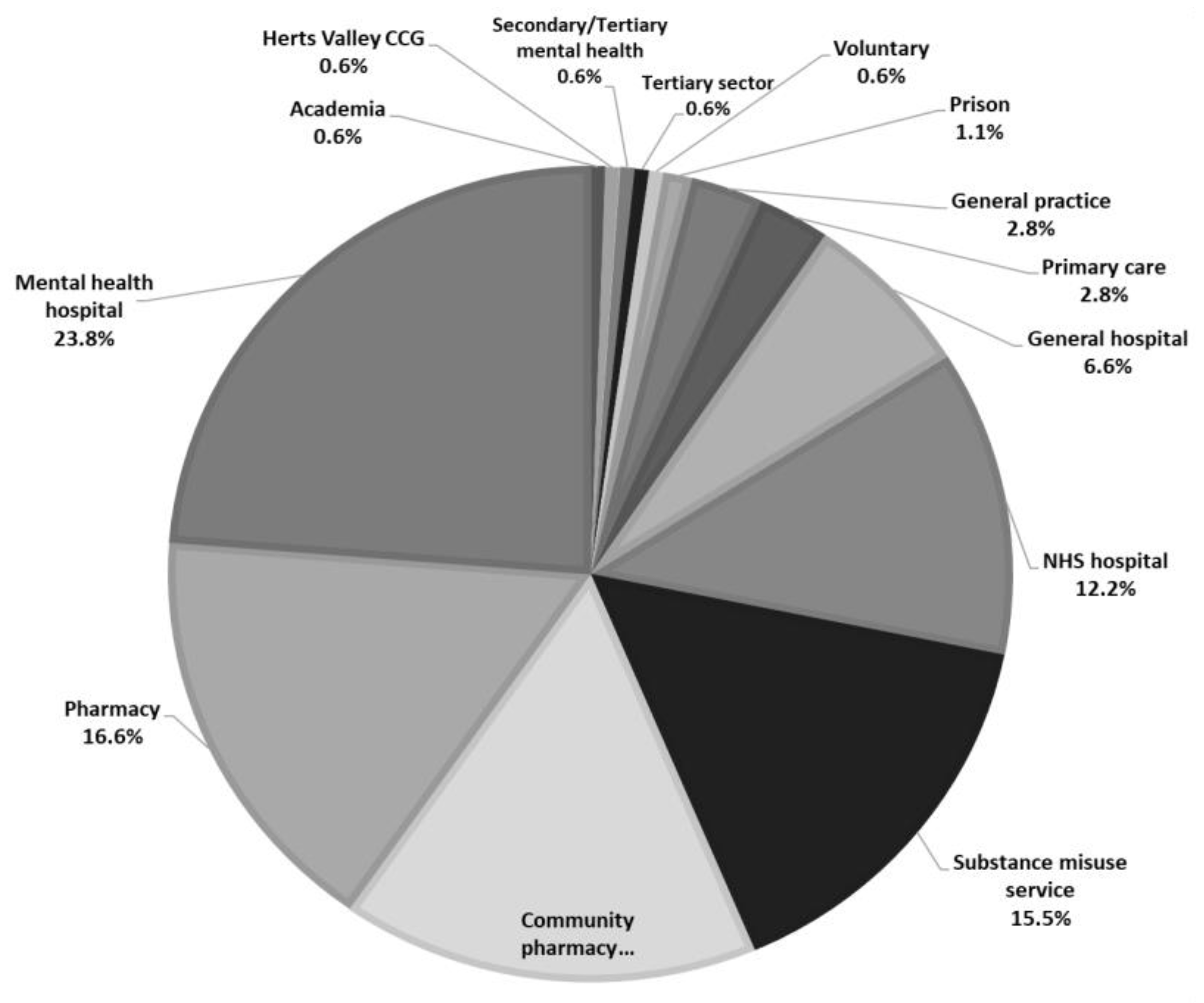
3.1. Participants
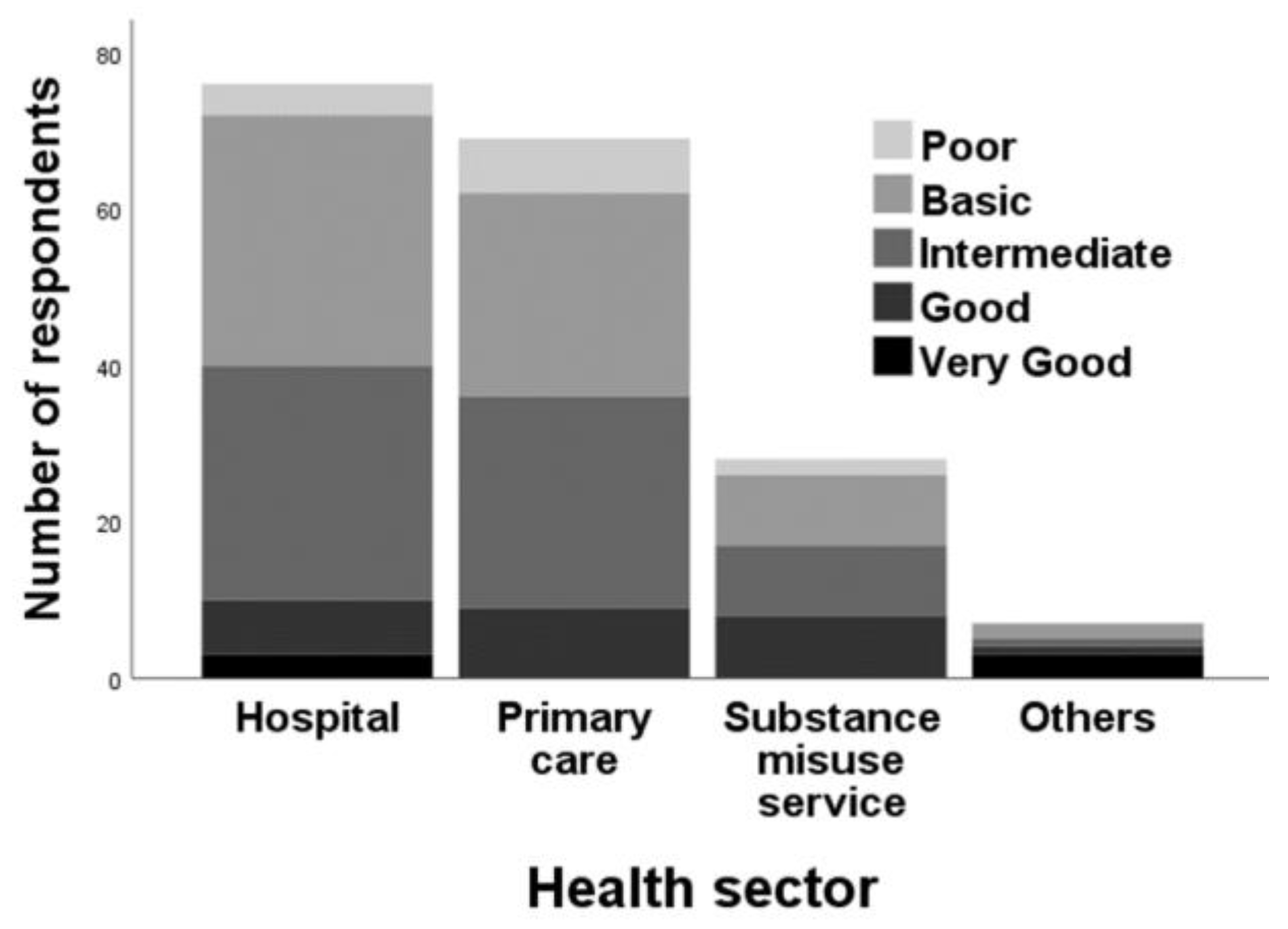
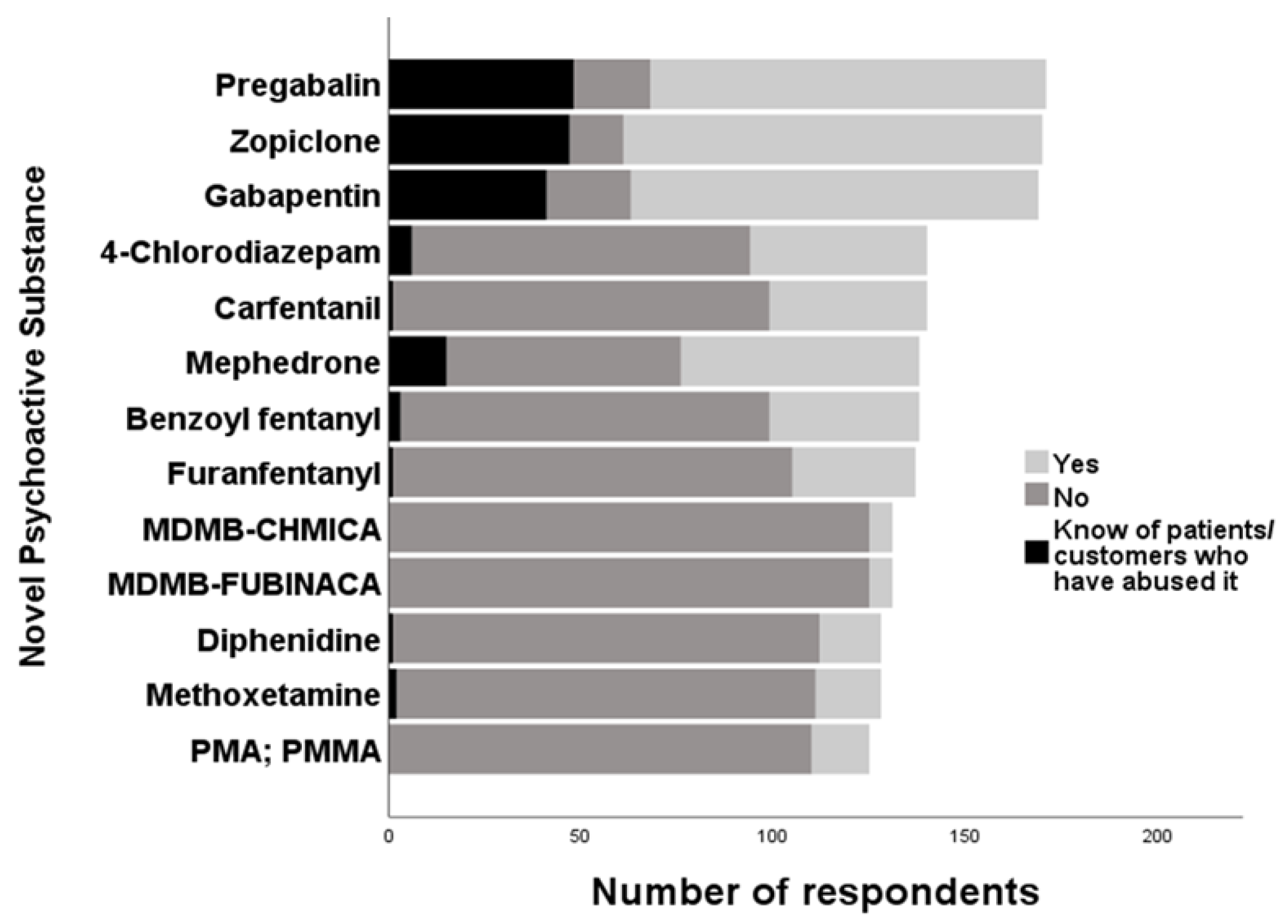
3.2. Knowledge of NPS
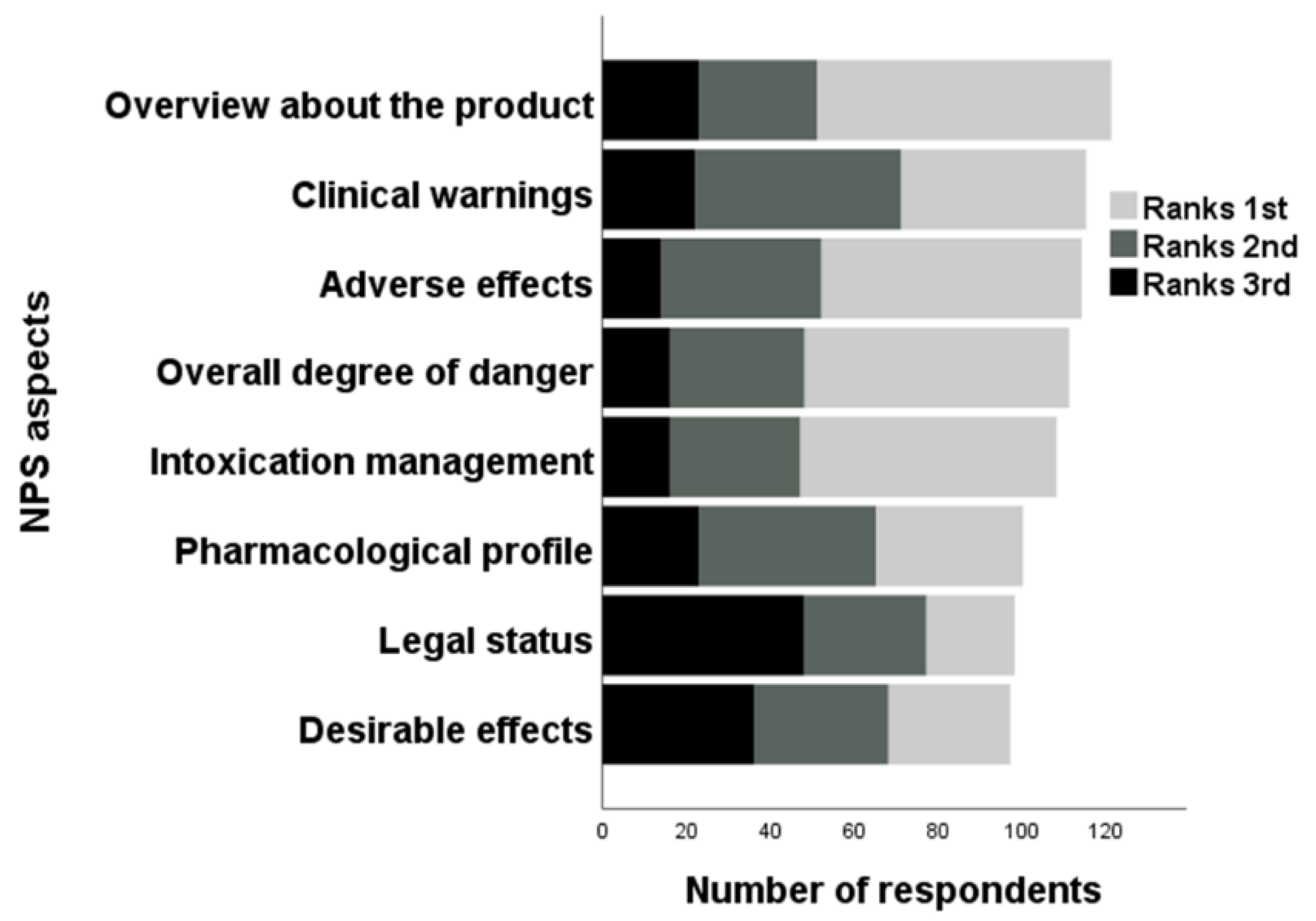
3.3. Relevance of NPS to HCPs
3.4. Feedback from Educational Training and Future Learning Needs
4. Discussion
4.1. Characteristics of HCPs
4.2. NPS Types
4.3. Educational Sessions’ Feedback
4.4. Conceptualisation of an Evidence-Informed Public Health Approach to NPS use in the UK
4.5. Implications and Recommendations for Policy-making and Clinical Practice
4.6. Limitations of Research and Suggestions for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethics Statement
References
- UNODC. The Challenge of New Psychoactive Substances; United Nation Office on Drugs and Crime: Vienna, Austria, 2013. Available online: https://www.unodc.org/documents/scientific/NPS_2013_SMART.pdf (accessed on 19 September 2019).
- EMCDDA-Europol. The state of the drugs problem in Europe—Annual report 2012; Publications Office of the European Union: Luxembourg; Available online: http://www.emcdda.europa.eu/attachements.cfm/att_190854_EN_TDAC12001ENC_.pdf (accessed on 19 September 2019).
- ACMD. Consideration of the Novel Psychoactive Substances (‘Legal Highs’); Advisory Council on the Misuse of Drugs, Home Office: London, UK, 2011. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/119139/acmdnps2011.pdf (accessed on 19 September 2019).
- Psychoactive Substances Act 2016; The Stationary Office Limited, 2016. Available online: https://www.legislation.gov.uk/ukpga/2016/2/pdfs/ukpga_20160002_en.pdf (accessed on 19 September 2019).
- Schifano, F. Recent Changes in Drug Abuse Scenarios: The New/Novel Psychoactive Substances (NPS) Phenomenon. Brain Sci. 2018, 8, 221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corkery, J.; Orsolini, L.; Papanti, D.; Schifano, F. Novel psychoactive substances (NPS) and recent scenarios: Epidemiological, anthropological and clinical pharmacological issues. In Light in Forensic Science: Issues and Applications; Royal Society of Chemistry: London, UK, 2018; Chapter 8; pp. 207–256. [Google Scholar]
- Goodair, C.M.; Corkery, J.; Claridge, H. Legal highs: A problem of definitions? Lett. Lancet 2014, 383, 1715. [Google Scholar] [CrossRef]
- Home Office. Review of the Psychoactive Substances Act 2016; Home Office: London, UK, 2018. Available online: https://www.gov.uk/government/publications/review-of-the-psychoactive-substances-act-2016 (accessed on 26 February 2020).
- Deligianni, E.; Daniel, O.J.; Corkery, J.M.; Schifano, F.; Lione, L. Impact of the UK Psychoactive Substances Act on awareness, use, experiences and knowledge of potential associated health risks of Novel Psychoactive Substances. Br. J. Clin. Pharmacol. 2019. [Google Scholar] [CrossRef] [PubMed]
- UNODC. UNODC World Drug Report; United Nations Office on Drugs and Crime: Vienna, Austria, 2018. Available online: https://www.unodc.org/LSS/announcement/Details/fa879924-6bdf-4ba2-a8eb-a87185d26439 (accessed on 19 September 2019).
- UNODC. UNODC-SMART: Almost 900 NPS Reported to UNODC from 119 countries and territories; United Nations Office on Drugs and Crime: Vienna, Austria, 2019. Available online: https://www.unodc.org/LSS/Announcement/Details/eff8dc38-7ab0-42b0-8cd9-753b89953fcc (accessed on 19 September 2019).
- Dignam, G.; Bigham, C. Novel psychoactive substances: A practical approach to dealing with toxicity from legal highs. BJA Educ. 2017, 17, 172–177. [Google Scholar] [CrossRef] [Green Version]
- Winstock, A.; Barratt, M.; Maier, L.; Aldridge, A.; Zhuparis, A.; Davies, E.; Ferris, J. Global Drug Survey (GDS) 2019 Key Findings Report. 2019. Available online: https://www.globaldrugsurvey.com/gds-2019/ (accessed on 26 February 2020).
- ONS. Deaths related to drug poisoning in England and Wales: 2018 registrations; Office for National Statistics: Newport, Gwent, 2019. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsrelatedtodrugpoisoninginenglandandwales/2018registrations/pdf (accessed on 19 September 2019).
- NRS. Drug-related Deaths in Scotland in 2018; National Records of Scotland: Edinburgh, Scotland, 2019. Available online: https://www.nrscotland.gov.uk/files//statistics/drug-related-deaths/2018/drug-related-deaths-18-pub.pdf (accessed on 19 September 2019).
- Webb, N.E.; Wood, D.M.; Greene, S.L.; Hunter, L.J.; Archer, J.R.H.; Dines, A.M.; Dargan, P.I. Change in the new psychoactive substances associated with Emergency Department acute toxicity presentations associated with the introduction of the UK 2016 Psychoactive Substances Act. Clin. Toxicol. 2019, 57, 36–41. [Google Scholar] [CrossRef]
- Henshall, D.E.; Innes, C.W.; Morrison, S.R.; Wilson, B.; Brown, R.A.; McAllister, S.M.; Reda, E. A prospective observational study of emergency department presentations following novel psychoactive substance use. Scott. Med. J. 2018, 63, 39–44. [Google Scholar] [CrossRef]
- EMCDDA. Fentanils and Synthetic Cannabinoids: Driving Greater Complexity into the Drug Situation; European Monitoring Centre for Drugs and Drug Addiction: Lisbon, Portugal, 2018. Available online: http://www.emcdda.europa.eu/system/files/publications/8870/2018-2489-td0118414enn.pdf (accessed on 19 September 2019).
- Janssen, P.A. Potent, new analgesics, tailor-made for different purposes. Acta Anaesthesiol. Scand. 1982, 26, 262–268. [Google Scholar] [CrossRef]
- WHO. Carfentanil Critical Review Report Agenda Item 4.8 Expert Committee; World Health Organisation: Geneva, Switzerland, 2017; Available online: https://www.who.int/medicines/access/controlled-substances/Critical_Review_Carfentanil.pdf (accessed on 26 February 2020).
- Baumann, M.H.; Majumdar, S.; Le Rouzic, V.; Hunkele, A.; Uprety, R.; Huang, X.P.; Pasternak, G.W. Pharmacological characterization of novel synthetic opioids (NSO) found in the recreational drug marketplace. Neuropharmacology 2018, 134, 101–107. [Google Scholar] [CrossRef]
- Schifano, F.; Chiappini, S.; Corkery, J.M.; Guirguis, A. Assessing the 2004–2018 Fentanyl Misusing Issues Reported to an International Range of Adverse Reporting Systems. Front. Pharmacol. 2019, 10, 1–10. [Google Scholar] [CrossRef]
- Martinotti, G.; Cinosi, E.; Santacroce, R.; Papanti, D.; Pasquini, A.; Mancini, V.; erino del Villar, C. Substance-related psychopathology and aggressiveness in a nightlife holiday resort: Results from a pilot study in a psychiatric inpatient unit in Ibiza. Hum. Psychopharmacol. 2017, 32, 2586. [Google Scholar] [CrossRef]
- Shafi, A.; Gallagher, P.; Stewart, N.; Martinotti, G.; Corazza, O. The risk of violence associated with novel psychoactive substance misuse in patients presenting to acute mental health services. Hum. Psychopharmacol. Clin. Exp. 2017, 32, e2606. [Google Scholar] [CrossRef] [PubMed]
- EMCDDA. European Drug Report Trends and Developments; European Monitoring Centre for Drugs and Drug Addiction: Lisbon, Portugal, 2018. Available online: http://www.emcdda.europa.eu/system/files/publications/8585/20181816_TDAT18001ENN_PDF.pdf (accessed on 19 September 2019).
- Fujita, Y.; Koeda, A.; Fujino, Y.; Onodera, M.; Kikuchi, S.; Niitsu, H.; Inoue, Y. Clinical and toxicological findings of acute intoxication with synthetic cannabinoids and cathinones. Acute Med. Surg. 2016, 3, 230–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdulrahim, D.; Bowden-Jones, O.; On behalf of the NEPTUNE Group. Guidance on the Clinical Management of Acute and Chronic Harms of Club Drugs and Novel Psychoactive Substances; The Health Foundation: London, UK, 2015; Available online: http://neptune-clinical-guidance.co.uk/wp-content/uploads/2015/03/NEPTUNE-Guidance-March-2015.pdf (accessed on 19 September 2019).
- Bourne, A.; Reid, D.; Hickson, F.; Torres-Rueda, S.; Weatherburn, P. Illicit drug use in sexual settings (‘chemsex’) and HIV/STI transmission risk behaviour among gay men in South London: Findings from a qualitative study. Sex. Transm. Infect. 2015, 91, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Bourne, A.; Reid, D.; Hickson, F.; Torres-Rueda, S.; Steinberg, P.; Weatherburn, P. “Chemsex” and harm reduction need among gay men in South London. Int. J. Drug Policy 2015, 26, 1171–1176. [Google Scholar] [CrossRef] [PubMed]
- Chiappini, S.; Schifano, F. A Decade of Gabapentinoid Misuse: An Analysis of the European Medicines Agency’s ‘Suspected Adverse Drug Reactions’ Database. CNS Drugs 2016, 30, 647–654. [Google Scholar] [CrossRef] [Green Version]
- Daly, C.; Griffin, E.; Ashcroft, D.M.; Webb, R.T.; Perry, I.J.; Arensman, E. Intentional Drug Overdose Involving Pregabalin and Gabapentin: Findings from the National Self-Harm Registry Ireland, 2007–2015. Clin. Drug Investig. 2018, 38, 373–380. [Google Scholar] [CrossRef]
- Reeves, R.R.; Ladner, M.E. Potentiation of the Effect of Buprenorphine/Naloxone With Gabapentin or Quetiapine. Am. J. Psychiatry 2014, 171, 691. [Google Scholar] [CrossRef]
- EMCDDA. The misuse of benzodiazepines among high-risk opioid users in Europe; European Monitoring Centre for Drugs and Drug Addiction: Lisbon, Portugal, 2018. Available online: http://www.emcdda.europa.eu/system/files/publications/2733/Misuse%20of%20benzos_POD2015.pdf (accessed on 26 February 2020).
- Johnson, C.F.; Barnsdale, L.R.; McAuley, A. Investigating the role of benzodiazepines in drug-related mortality: A systematic review undertaken on behalf of The Scottish National Forum on Drug-Related Deaths. 2016. Available online: https://dspace.stir.ac.uk/handle/1893/23220#.XCtFKlz7TtQ (accessed on 19 September 2019).
- Manchester, K.R.; Lomas, E.C.; Waters, L.; Dempsey, F.C.; Maskell, P.D. The emergence of new psychoactive substance (NPS) benzodiazepines: A review. Drug Test. Anal. 2018, 10, 37–53. [Google Scholar] [CrossRef] [Green Version]
- NRS. Drug-related deaths in Scotland 2016; National Records of Scotland: Edinburgh, Scotland, 2017. Available online: https://www.nrscotland.gov.uk/files//statistics/drug-related-deaths/drd2016/drug-related-deaths-16-pub.pdf (accessed on 19 September 2019).
- NRS. Drug-related deaths in Scotland in 2017; National Records of Scotland: Edinburgh, Scotland, 2018. Available online: https://www.nrscotland.gov.uk/files/statistics/drug-related-deaths/17/drug-related-deaths-17-pub.pdf (accessed on 19 September 2019).
- Campbell, A.; O Neill, N.; Higgins, K. Health and Social Care workers’ perceptions of NPS use in Northern Ireland. Int. J. Drug Policy 2017, 40, 93–101. [Google Scholar] [CrossRef]
- Gittins, R.; Guirguis, A.; Schifano, F.; Maidment, I. Exploration of the use of new psychoactive substances by individuals in treatment for substance misuse in the UK. Brain Sci. 2018, 8, 58. [Google Scholar] [CrossRef] [Green Version]
- Guirguis, A.; Corkery, J.M.; Stair, J.L.; Kirton, S.; Zloh, M.; Goodair, C.M.; Davidson, C. Survey of knowledge of legal highs (novel psychoactive substances) amongst London pharmacists. Drugs Alcohol Today 2015, 15, 93–99. [Google Scholar] [CrossRef] [Green Version]
- Hughes, E.; Bressington, D.; Sharratt, K.; Gray, R. Novel psychoactive substance use by mental health service consumers: An online survey of inpatient health professionals’ views and experiences. Adv. Dual Diagn. 2018, 11, 30–39. [Google Scholar] [CrossRef]
- Owie, R.E.; Gosney, P.; Roney, A.; O’brien, A. Psychiatrists’ knowledge of novel psychoactive substances. Drugs Alcohol Today 2017, 17, 178–185. [Google Scholar] [CrossRef]
- Wood, D.M.; Ceronie, B.; Dargan, P.I. Healthcare professionals are less confident in managing acute toxicity related to the use of new psychoactive substances (NPS) compared with classical recreational drugs. QJM 2016, 109, 527–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonato, P.; Corazza, O.; Santonastaso, P.; Corkery, J.; Deluca, P.; Davey, Z.; Schifano, F. Novel psychoactive substances as a novel challenge for health professionals: Results from an Italian survey. Hum. Psychopharmacol. Clin. Exp. 2013, 28, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Corazza, O.; Assi, S.; Trincas, G.; Simonato, G.; Corkery, J.; Davey, Z.; Deluca, P. Novel Drugs, Novel Solutions: Exploring the potential of technological tools for prevention of drug abuse. Ital. J. Addict. 2011, 1, 25–30. [Google Scholar]
- ReDNet Research Group. Le nuove potenzialità della prevenzione digitale in materia di nuove droghe—Research Database—University of Hertfordshire. Dipendenze Patologiche. 2010. Available online: http://researchprofiles.herts.ac.uk/portal/en/publications/le-nuove-potenzialita-della-prevenzione-digitale-in-materia-di-nuove-droghe(e4511105-5c1d-479f-b9ea-e6bea4e489c7)/export.html (accessed on 19 September 2019).
- Tracy, D.K.; Wood, D.M.; Baumeister, D. Novel psychoactive substances: Identifying and managing acute and chronic harmful use. BMJ (Clin. Res. Ed.) 2017, 356, 6814. [Google Scholar] [CrossRef] [Green Version]
- Tracy, D.K.; Wood, D.M.; Baumeister, D. Novel psychoactive substances: Types, mechanisms of action, and effects. BMJ (Clin. Res. Ed.) 2017, 356, 6848. [Google Scholar] [CrossRef] [Green Version]
- EMCDDA-Europol. EMCDDA–Europol 2017 Annual Report on the implementation of Council Decision 2005/387/JHA; European Monitoring Centre for Drugs and Drug Addiction: Lisbon, Portugal, 2017. Available online: http://www.emcdda.europa.eu/system/files/publications/9282/20183924_TDAN18001ENN_PDF.pdf (accessed on 19 September 2019).
- Macleod, S. Likert Scale. Simply Psychology. 2008. Available online: https://www.simplypsychology.org/likert-scale.html (accessed on 19 September 2019).
- Guirguis, A.; Hawksworth, G.; Bond, C.; Lawrence, J.; Martini, L.G. New Psychoactive Substances: A Guide for Pharmacists; Royal Pharmaceutical Society: London, UK, 2018; Available online: https://www.rpharms.com/Portals/0/RPS%20document%20library/Open%20access/Science/RPS%20NPS%20Fact%20sheet.pdf?ver=2018-06-18-141822-160 (accessed on 19 September 2019).
- Batisse, A.; Grégoire, M.; Marillier, M.; Fortias, M.; Djezzar, S. Usage de cathinones à Paris. L’Encéphale 2016, 42, 354–360. [Google Scholar] [CrossRef]
- Schifano, F.; Leoni, M.; Martinotti, G.; Rawaf, S.; Rovetto, F. Importance of cyberspace for the assessment of the drug abuse market: Preliminary results from the Psychonaut 2002 project. Cyberpsychology Behav. 2003, 6, 405–410. [Google Scholar] [CrossRef]
- Ralphs, R.; Gray, P. New psychoactive substances: New service provider challenges. Drugs Educ. Prev. Policy 2018, 25, 301–312. [Google Scholar] [CrossRef]
- Schifano, F.; Chiappini, S.; Corkery, J.M.; Guirguis, A. An Insight into Z-Drug Abuse and Dependence: An Examination of Reports to the European Medicines Agency Database of Suspected Adverse Drug Reactions. Int. J. Neuropsychopharmacol. 2019, 22, 270–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, J.M.; Irvine, R.J. Mechanisms of fatal opioid overdose. Addiction (Abingdon Engl.) 1999, 94, 961–972. [Google Scholar] [CrossRef]
- Schifano, F.; Chiappini, S.; Corkery, J.M.; Guirguis, A. Abuse of prescription drugs in the context of novel psychoactive substances (NPS): A systematic review. Brain Sci. 2018, 8, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cairns, R.; Schaffer, A.L.; Ryan, N.; Pearson, S.; Buckley, N.A. Rising pregabalin use and misuse in Australia: Trends in utilization and intentional poisonings. Addiction 2019, 114, 1026–1034. [Google Scholar] [CrossRef] [PubMed]
- Schifano, F.; Chiappini, S. Pregabalin: A range of misuse-related unanswered questions. CNS Neurosci. Ther. 2019, 25, 659–660. [Google Scholar] [CrossRef] [Green Version]
- Winstock, A.; Barratt, M.; Maier, L.; Aldridge, A.; Zhuparis, A.; Davies, E.; Ferris, J. Global Drug Survey (GDS) 2018 Key Findings Report. 2018. Available online: https://www.globaldrugsurvey.com/gds-2018/ (accessed on 26 February 2020).
- Hikin, L.; Smith, P.R.; Ringland, E.; Hudson, S.; Morley, S.R. Multiple fatalities in the North of England associated with synthetic fentanyl analogue exposure: Detection and quantitation a case series from early 2017. Forensic Sci. Int. 2018, 282, 179–183. [Google Scholar] [CrossRef]
- Abdulrahim, D.; Bowden-Jones, O. The Misuse of Synthetic Opioids: Harms and Clinical Management of Fentanyl, Fentanyl Analogues and Other Novel Synthetic Opioids Information for Clinicians; The Health Foundation: London, UK, 2018; Available online: http://neptune-clinical-guidance.co.uk/wp-content/uploads/2018/03/The-misuse-of-synthetic-opioids.pdf (accessed on 19 September 2019).
- Bourne, A.; Reid, D.; Hickson, F.; Torres, S.; Weatherburn, R.P. The Chemsex Study: Drug Use in Sexual Settings Among Gay and Bisexual Men in Lambeth, Southwark and Lewisham; Sigma Research, London School of Hygiene & Tropical Medicine, 2014. Available online: https://www.lambeth.gov.uk/sites/default/files/ssh-chemsex-study-final-main-report.pdf (accessed on 19 September 2019).
- Keogh, P.; Reid, D.; Bourne, A.; Weatherburn, P.; Hickson, F.; Jessup, K.; Hammond, G. Wasted Opportunities: Problematic Alcohol and Drug Use among Gay Men and Bisexual Men; Sigma Research, London School of Hygiene & Tropical Medicine, 2009; Available online: http://researchonline.lshtm.ac.uk/1408/ (accessed on 19 September 2019).
- Sample, I. ‘Superman’ pill deaths spark calls for dangerous-drugs alert system. The Guardian. 2015. Available online: https://www.theguardian.com/society/2015/jan/16/superman-pill-deaths-dangerous-drugs-alert-system (accessed on 19 September 2019).
- Guirguis, A.; Corkery, J.M.; Stair, J.L.; Zloh, M.; Kirton, S.B.; Schifano, F. Intended and unintended use of cathinone mixtures. J. Hum. Psychopharmacol. Clin. Exp. 2017, 32. [Google Scholar] [CrossRef]
- Hillebrand, J.; Olszewski, D.; Sedefov, R. Legal Highs on the Internet. Subst. Use Misuse 2010, 45, 330–340. [Google Scholar] [CrossRef]
- Simolka, K.; Lindigkeit, R.; Schiebel, H.-M.; Papke, U.; Ernst, L.; Beuerle, T. Analysis of synthetic cannabinoids in “spice-like” herbal highs: Snapshot of the German market in summer 2011. Anal. Bioanal. Chem. 2012, 404, 157–171. [Google Scholar] [CrossRef]
- Guirguis, A.; Hawksworth, G.; Bond, C.; Lawrence, J.M.; Martini, L.G. New psychoactive substances. In Quick Reference Guides; Royal Pharmaceutical Society: London, UK, 2018; Available online: https://www.rpharms.com/resources/quick-reference-guides/new-psychoactive-substances (accessed on 19 September 2019).
- World Health Organization. Technical Series on Safer Primary Care. Education and Training: Technical Series on Safer Primary Care; World Health Organization: Geneva, Switzerland, 2016; ISBN 978-92-4-151160-5. [Google Scholar]
- EMCDDA. Health Responses to New Psychoactive Substances; European Monitoring Centre for Drugs and Drug Addiction: Lisbon, Portugal, 2016. Available online: http://www.emcdda.europa.eu/system/files/publications/2812/TD0216555ENN.pdf (accessed on 19 September 2019).
- Meader, N.; Mdege, N.; McCambridge, J. The public health evidence-base on novel psychoactive substance use: Scoping review with narrative synthesis of selected bodies of evidence. J. Public Health (Oxf. Engl.) 2018, 40, e303–e319. [Google Scholar] [CrossRef] [PubMed]
- UNODC. Market Analysis of Synthetic Drugs. Amphetamine-Type Stimulants, New Psychoactive Substances. World Drug Report 2017; United Nations Office on Drugs and Crime: Vienna, Austria, 2017. Available online: http://www.unodc.org/documents/scientific/Booklet_4_Market_Analysis_of_Synthetic_Drugs_ATS_NPS.pdf (accessed on 19 September 2019).
- Guirguis, A. New psychoactive substances: A public health issue. Int. J. Pharm. Pract. 2017, 25, 323–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EMCDDA. Health and Social Responses to Drug Problems. A European Guide; European Monitoring Centre for Drugs and Drug Addiction: Lisbon, Portugal, 2017. Available online: https://publications.europa.eu/en/publication-detail/-/publication/d8574d27-ae31-11e7-837e-01aa75ed71a1/language-en (accessed on 19 September 2019).
- Strang, J.; Babor, T.; Caulkins, J.; Fischer, B.; Foxcroft, D.; Humphreys, K. Drug policy and the public good: Evidence for effective interventions. Lancet 2012, 379, 71–83. [Google Scholar] [CrossRef]
- PHE. New Psychoactive Substances (A toolkit for Substance Misuse Commissioners); Public Health England: London, UK, 2014. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/669429/nps-a-toolkit-for-substance-misuse-commissioners.pdf (accessed on 19 September 2019).
- Guirguis, A.; Lawrence, M.J. New Psychoactive Substances (NPS). In Medicines, Ethics and Practice. The Professional Guide for Pharmacists, 41st ed.; Tang, W., Ed.; Royal Pharmaceutical Society: London, UK, 2017; pp. 90–91. [Google Scholar]
- Royal Pharmaceutical Society. Medicines, Ethics and Practice (MEP) 43. 2019. Available online: https://www.rpharms.com/resources/publications/medicines-ethics-and-practice-mep (accessed on 19 September 2019).
- Helander, A.; Beck, O.; Hägerkvist, R.; Hultén, P. Identification of novel psychoactive drug use in Sweden based on laboratory analysis—Initial experiences from the STRIDA project. Scand. J. Clin. Lab. Investig. 2013, 73, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Burns, C. First Home Office-licensed street drug-testing clinic opens. Pharm. J. 2019, 302, 7923. [Google Scholar]
- Chary, M.; Yi, D.; Manini, A.F. Candyflipping and Other Combinations: Identifying Drug-Drug Combinations from an Online Forum. Front. Psychiatry 2018, 9, 135–144. [Google Scholar] [CrossRef]
- Alotaibi, M.R.; Husbands, S.M.; Blagbrough, I.S. 1H, 13C, 15N HMBC, and 19F NMR spectroscopic characterisation of seized flephedrone, cut with benzocaine. J. Pharm. Biomed. Anal. 2015, 107, 535–538. [Google Scholar] [CrossRef] [Green Version]
- Kavanagh, P.; O’Brien, J.; Fox, J.; O’Donnell, C.; Christie, R.; Power, J.D.; McDermott, S.D. The analysis of substituted cathinones. Part 3. Synthesis and characterisation of 2,3-methylenedioxy substituted cathinones. Forensic Sci. Int. 2012, 216, 19–28. [Google Scholar] [CrossRef]
- Zuba, D.; Byrska, B. Prevalence and co-existence of active components of “legal highs.”. Drug Test. Anal 2013, 5, 420–429. [Google Scholar] [CrossRef]
- Zamengo, L.; Frison, G.; Bettin, C.; Sciarrone, R. Understanding the risks associated with the use of new psychoactive substances (NPS): High variability of active ingredients concentration, mislabelled preparations, multiple psychoactive substances in single products. Toxicol. Lett. 2014, 229, 220–228. [Google Scholar] [CrossRef]
- Guirguis, A. Novel psychoactive substances: Understanding the new illegal drug market. Clin. Pharm. 2018, 10, 1116. [Google Scholar] [CrossRef] [Green Version]
- Schifano, F.; Chiappini, S. Is there such a thing as a “lope” dope? Analysis of loperamide-related European Medicines Agency (EMA) pharmacovigilance database reports. PLoS ONE 2018, 13, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schifano, F.; Papanti, G.D.; Orsolini, L.; Corkery, J.M. The consequences of drug misuse on post-marketing surveillance. Expert Rev. Clin. Pharmacol. 2016, 9, 867–871. [Google Scholar] [CrossRef] [Green Version]
- Lavallée, J.F.; Gray, T.A.; Dumville, J.; Russell, W.; Cullum, N. The effects of care bundles on patient outcomes: A systematic review and meta-analysis. Implement. Sci. 2017, 12, 142. [Google Scholar] [CrossRef] [PubMed]
- Abdulrahim, D.; Bowden-Jones, O. Harms of Synthetic Cannabinoid Receptor Agonists (SCRAs) and Their Management; The Health Foundation: London, UK, 2016; Available online: http://neptune-clinical-guidance.co.uk/wp-content/uploads/2016/07/Synthetic-Cannabinoid-Receptor-Agonists.pdf (accessed on 19 September 2019).
- Adley, M. The Drugs Wheel. Version 2.0.6. 2018. Available online: http://www.thedrugswheel.com/ (accessed on 16 April 2019).
- Bersani, F.S.; Corazza, O.; Albano, G.; Valeriani, G.; Santacroce, R.; Bolzan Mariotti Posocco, F.; Schifano, F. 25C-NBOMe: Preliminary data on pharmacology, psychoactive effects, and toxicity of a new potent and dangerous hallucinogenic drug. Biomed Res. Int. 2014, 2014, 734749. [Google Scholar] [CrossRef] [PubMed]
- Martinotti, G.; Lupi, M.; Acciavatti, T.; Cinosi, E.; Santacroce, R.; Signorelli, M.S.; Alvin di Giannantonio, M. Novel psychoactive substances in young adults with and without psychiatric comorbidities. Biomed Res. Int. 2014, 2014, 815424. [Google Scholar] [CrossRef]
- Vento, A.E.; Martinotti, G.; Cinosi, E.; Lupi, M.; Acciavatti, T.; Carrus, D.; Schifano, F. Substance Use in the Club Scene of Rome: A Pilot Study. Biomed Res. Int. 2014, 2014, 617546. [Google Scholar] [CrossRef]
- Independent Expert Working Group. Drug Misuse and Dependence: UK Guidelines on Clinical Management; Department of Health: London, UK, 2017. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/673978/clinical_guidelines_2017.pdf (accessed on 19 September 2019).
- Schifano, F.; Chiappini, S. Is there a potential of misuse for venlafaxine and bupropion? Front. Pharmacol. 2018, 9, 239. [Google Scholar] [CrossRef] [Green Version]
- Etikan, I.; Musa, S.A.; Alkassim, R.S. Comparison of Convenience Sampling and Purposive Sampling. Am. J. Theor. Appl. Stat. 2016, 5, 1. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Positive Response: Number Out of Total (%) | |||||
|---|---|---|---|---|---|
| Hospital | Primary Care | Substance Misuse Service | Others | p-Value | |
| Good/very good level of knowledge | 11/77 (14.3) | 8/68 (11.8) | 8/28 (28.6) | 4/7 (57.1) | 0.008 * |
| Provide advice/counselling | 40/72 (55.6) | 20/55 (36.4) | 19/26 (73.1) | 4/4 (100.0) | 0.002 * |
| Fairly/very confident about providing advice | 34/77 (44.2) | 21/68 (30.9) | 15/28 (53.6) | 5/7 (71.4) | 0.051 * |
| Encounter customers/patients seeking advice | 22/76 (28.9) | 8/68 (11.8) | 13/28 (46.4) | 5/7 (71.4) | < 0.001 |
| Fairly/very confident about providing advice on adverse effects | 17/72 (23.6) | 11/63 (17.5) | 14/28 (50.0) | 4/7 (57.1) | 0.003 |
| Knowledge on NPS/legal highs fairly/very significant in work | 58/68 (85.3) | 40/57 (70.2) | 24/26 (92.3) | 5/6 (83.3) | 0.058 * |
| Positive Response: Number Out of Total (%) | |||||
|---|---|---|---|---|---|
| GP | Nurse | Pharmacist | Others | p-Value | |
| Good/very good level of knowledge | 0/17 (0.0) | 10/50 (20.0) | 16/106 (15.1) | 4/12 (33.3) | 0.086 * |
| Provide advice/counselling | 8/16 (50.0) | 38/48 (79.2) | 31/90 (34.4) | 5/6 (83.3) | <0.001 * |
| Fairly/very confident about providing advice | 4/17 (23.5) | 28/50 (56.0) | 35/105 (33.3) | 6/12 (50.0) | 0.021 |
| Encounter customers/patients seeking advice | 5/17 (29.4) | 21/50 (42.0) | 19/104 (18.3) | 4/12 (33.3) | 0.018 * |
| Fairly/very confident about providing advice on adverse effects | 3/16 (18.8) | 21/49 (42.9) | 18/97 (18.6) | 2/10 (20.0) | 0.013 * |
| Knowledge on NPS/legal highs fairly/very significant in work | 10/17 (58.8) | 41/46 (89.1) | 69/87 (79.3) | 8/9 (88.9) | 0.052 * |
| Participant | Response |
|---|---|
| Nurse, mental health hospital | “It is an issue that still has elements of being unclear as what is legal and what is now illigel [sic], however the increase and potency of the drug on the street makes it an issue that affects all aspects of society.” |
| Pharmacist, substance misuse service | “NPS are not going away—and if anything, are going to get more designer and specific—we need to have understanding of their basics so we can formulate a base line approach as names and formulas change.” |
| General practitioner, general practice | “should be taught in schools about dangers of these. Use in universities seems very high” |
| Family safeguard worker, substance misuse service | “Please implement training as soon as possible. It is much needed to keep abreast of information and dangers on current legal highs.” |
| Pharmacist, community | “We have a significant problem with customers wanting to purchase codeine products in excess. These people are addicted to it but the only place to refer them to is the RISE addiction team who are overworked already.” |
| Participant | Response |
|---|---|
| GP 1 | “Abuse of medications I didn’t realise had abuse potential; pharmacokinetics of Gaba meds/opiates & withdrawal of Benzos.” |
| GP 2 | “misuse of prescriber drugs such as tramadol & fentanyl patch.” |
| GP 3 | “Pregabalin/Gabapentin have high abuse potential.” |
| GP 4 | “Massive growth in NPS. Actually feel helpless against this! I ran an EMIS search immediately. We have 5 ppl (out of 14000) on repeat for fentanyl patches. I’ll write to all regarding safe disposal.” |
| GP 5 | “The pharmacodynamic pathways were really well explained & all makes a lot more sense again!; The number of potency of NPS’s -very scary.; The prevalence of NPS in herbal/food supps.” |
| GP 6 | “Lots of things about NPS; RIDR; how various drugs are abused and dangers of withdrawal.” |
| GP 7 | “The pharmacodynamic pathways were really well explained & it all makes a lot more sense again!” |
| Participant | Response |
|---|---|
| Ph 1 | “Naloxone isn’t always suitable antagonist for NPS; Drug wars and NPS are very prevalent; Drug tests miss a lot of drugs of abuse…” |
| Ph 2 | “Different classes of NPS; New substances being introduced all the time-not always detected; Rx drugs misused—gabapentin, pregabalin, venlafaxine.” |
| Ph 3 | “How to educate patients on NPS; Different types of NPS; Potential drugs that can be abused (e.g., POMs).” |
| Ph 5 | “NPS market, NPS user groups; What can we do? Harm reduction, awareness …” |
| Ph 6 | “What NPS drugs; How dangerous NPS drugs are and the harm they can cause; Didn’t know before the presentation: Buscopan, Gabapentin, Pregabalin can be abused …” |
| Ph 8 | “Challenges re using NPS-adverse reactions/toxicity/fatalities; Scale of the problem—in terms of use/difficulty monitoring; How quickly NPS are changing/its limitations in research …” |
| Participant | Response |
|---|---|
| Ph 4 | “more updates….. on new drugs of abuse both legal POMs Ps etc… and illicit” |
| Ph 9 | “Extremely informative & interesting session” |
| Ph 10 | “Regular talks to update us on them!” |
| Ph 20 | “To have more trainings, talks, workshops & to include also recovery workers; perhaps an NPS representative/head?” |
| GP 8 | “Discussion/evidence on why people abuse meds. Discussion about…… drug addiction” |
| GP 9 | “update on alcohol abuse” |
| GP 10 | “Would be nice to have back to basic update + local services again some point” |
| GP 11 | “How to identify and treat drug overdose /withdrawal.” |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos, C.; Guirguis, A.; Smeeton, N.; Zaman, H.; Felice, A.-M.; Bancroft, S.; Gittins, R.; Hawksworth, G.; Corkery, J.M.; Schifano, F. Exploring the Baseline Knowledge and Experience of Healthcare Professionals in the United Kingdom on Novel Psychoactive Substances. Brain Sci. 2020, 10, 142. https://doi.org/10.3390/brainsci10030142
Ramos C, Guirguis A, Smeeton N, Zaman H, Felice A-M, Bancroft S, Gittins R, Hawksworth G, Corkery JM, Schifano F. Exploring the Baseline Knowledge and Experience of Healthcare Professionals in the United Kingdom on Novel Psychoactive Substances. Brain Sciences. 2020; 10(3):142. https://doi.org/10.3390/brainsci10030142
Chicago/Turabian StyleRamos, Camille, Amira Guirguis, Nigel Smeeton, Hadar Zaman, Anna-Marie Felice, Stephanie Bancroft, Rosalind Gittins, Gill Hawksworth, John Martin Corkery, and Fabrizio Schifano. 2020. "Exploring the Baseline Knowledge and Experience of Healthcare Professionals in the United Kingdom on Novel Psychoactive Substances" Brain Sciences 10, no. 3: 142. https://doi.org/10.3390/brainsci10030142