
Patterns of Healthcare Resource Utilisation of Critical Care Survivors between 2006 and 2017 in Wales: A Population-Based Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
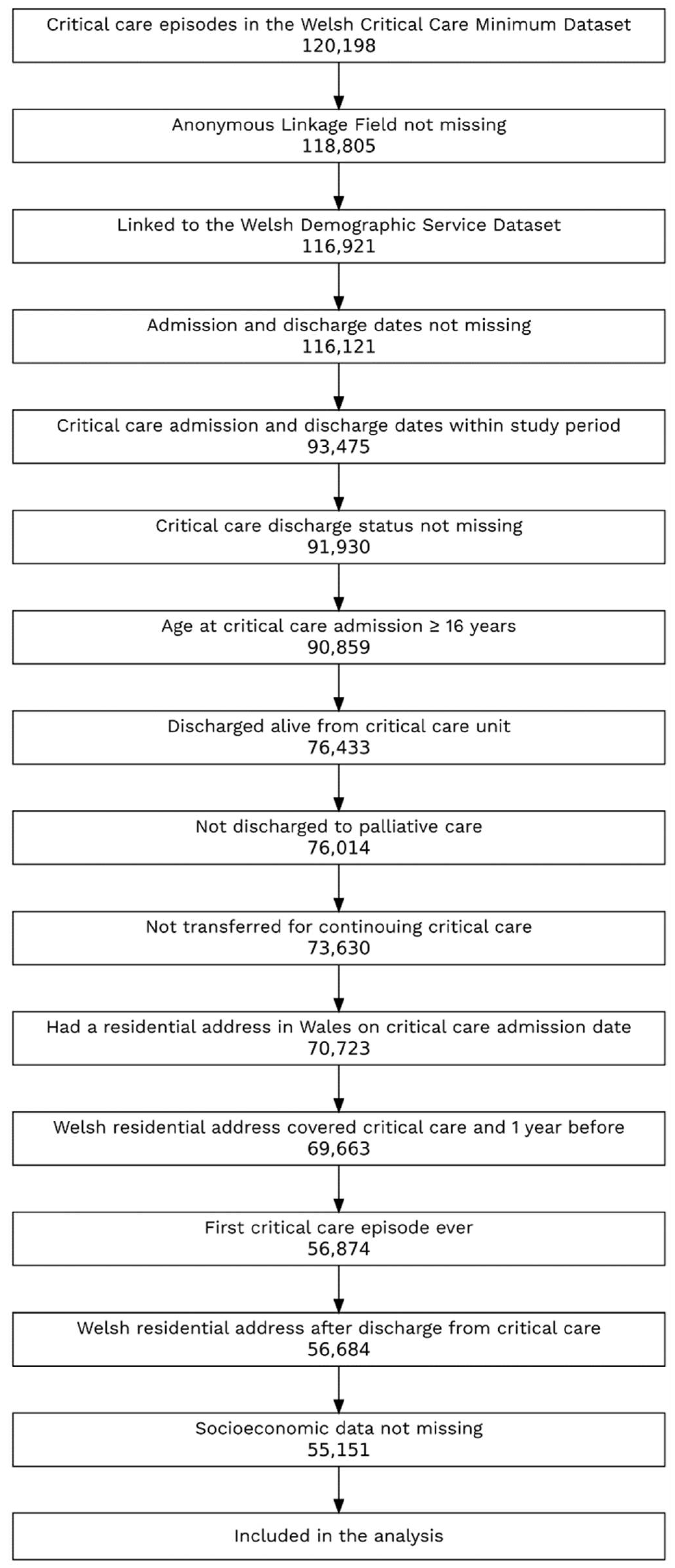
2.2. Patient Selection
2.3. Study Variables
2.4. Statistical Analysis
2.5. Reporting
3. Results
3.1. Demographics and Descriptive Analysis
3.2. Factors Associated with Post-Critical-Care HRU
3.3. Comparison with the Wider Hospital Population
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pandharipande, P.P.; Girard, T.D.; Jackson, J.C.; Morandi, A.; Thompson, J.L.; Pun, B.T.; Brummel, N.E.; Hughes, C.G.; Vasilevskis, E.E.; Shintani, A.K.; et al. Long-Term Cognitive Impairment after Critical Illness. N. Engl. J. Med. 2013, 369, 1306–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herridge, M.S.; Tansey, C.M.; Matté, A.; Tomlinson, G.; Diaz-Granados, N.; Cooper, A.; Guest, C.B.; Mazer, C.D.; Mehta, S.; Stewart, T.E.; et al. Functional Disability 5 Years after Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2011, 364, 1293–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, D.; Davidson, J.E.; Harvey, M.A.; Bemis-Dougherty, A.; Hopkins, R.O.; Iwashyna, T.J.; Wagner, J.; Weinert, C.; Wunsch, H.; Bienvenu, O.J.; et al. Exploring the Scope of Post-Intensive Care Syndrome Therapy and Care: Engagement of Non-Critical Care Providers and Survivors in a Second Stakeholders Meeting. Criti. Care Med. 2014, 42, 2518–2526. [Google Scholar] [CrossRef] [PubMed]
- Harvey, M.A.; Davidson, J.E. Postintensive Care Syndrome: Right Care, Right Now...and Later. Crit. Care Med. 2016, 44, 381–385. [Google Scholar] [CrossRef]
- Hill, A.D.; Fowler, R.A.; Pinto, R.; Herridge, M.S.; Cuthbertson, B.H.; Scales, D.C. Long-Term Outcomes and Healthcare Utilization Following Critical Illness–a Population-Based Study. Crit. Care 2016, 20, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hua, M.; Gong, M.N.; Brady, J.; Wunsch, H. Early and Late Unplanned Rehospitalizations for Survivors of Critical Illness. Crit. Care Med. 2015, 43, 430–438. [Google Scholar] [CrossRef] [Green Version]
- Lone, N.I.; Gillies, M.A.; Haddow, C.; Dobbie, R.; Rowan, K.M.; Wild, S.H.; Murray, G.D.; Walsh, T.S. Five-Year Mortality and Hospital Costs Associated with Surviving Intensive Care. Am. J. Respir. Crit. Care Med. 2016, 194, 198–208. [Google Scholar] [CrossRef] [Green Version]
- Desai, S.V.; Law, T.J.; Needham, D.M. Long-Term Complications of Critical Care. Crit. Care Med. 2011, 39, 371–379. [Google Scholar] [CrossRef]
- Iwashyna, T.J. Survivorship Will Be the Defining Challenge of Critical Care in the 21st Century. Ann. Intern. Med. 2010, 153, 204–205. [Google Scholar] [CrossRef]
- Szakmany, T.; Walters, A.M.; Pugh, R.; Battle, C.; Berridge, D.M.; Lyons, R.A. Risk Factors for 1-Year Mortality and Hospital Utilization Patterns in Critical Care Survivors: A Retrospective, Observational, Population-Based Data Linkage Study. Crit. Care Med. 2019, 47, 15–22. [Google Scholar] [CrossRef]
- Jouan, Y.; Grammatico-Guillon, L.; Teixera, N.; Hassen-Khodja, C.; Gaborit, C.; Salmon-Gandonnière, C.; Guillon, A.; Ehrmann, S. Healthcare Trajectories before and after Critical Illness: Population-Based Insight on Diverse Patients Clusters. Ann. Intensive Care 2019, 9, 126. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.; Brett, S.J.; Stokes, T. Rehabilitation after Critical Illness: Summary of NICE Guidance. BMJ 2009, 338, b822. [Google Scholar] [CrossRef] [PubMed]
- Lyons, R.A.; Jones, K.H.; John, G.; Brooks, C.J.; Verplancke, J.P.; Ford, D.V.; Brown, G.; Leake, K. The SAIL Databank: Linking Multiple Health and Social Care Datasets. BMC Med. Inf. Decis. Mak. 2009, 9, 3. [Google Scholar] [CrossRef] [Green Version]
- Ford, D.V.; Jones, K.H.; Verplancke, J.P.; Lyons, R.A.; John, G.; Brown, G.; Brooks, C.J.; Thompson, S.; Bodger, O.; Couch, T.; et al. The SAIL Databank: Building a National Architecture for e-Health Research and Evaluation. BMC Health Serv. Res. 2009, 9, 157. [Google Scholar] [CrossRef] [Green Version]
- Rodgers, S.E.; Demmler, J.C.; Dsilva, R.; Lyons, R.A. Protecting Health Data Privacy While Using Residence-Based Environment and Demographic Data. Health Place 2012, 18, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, S.E.; Lyons, R.A.; Dsilva, R.; Jones, K.H.; Brooks, C.J.; Ford, D.V.; John, G.; Verplancke, J.P. Residential Anonymous Linking Fields (RALFs): A Novel Information Infrastructure to Study the Interaction between the Environment and Individuals’ Health. J. Public Health 2009, 31, 582–588. [Google Scholar] [CrossRef] [Green Version]
- Bottle, A.; Aylin, P. Comorbidity Scores for Administrative Data Benefited from Adaptation to Local Coding and Diagnostic Practices. J. Clin. Epidemiol. 2011, 64, 1426–1433. [Google Scholar] [CrossRef]
- Welsh Index of Multiple Deprivation 2011 Technical Report; Welsh Government: Cardiff, Wales, 2011.
- Thayer, D.; Rees, A.; Kennedy, J.; Collins, H.; Harris, D.; Halcox, J.; Ruschetti, L.; Noyce, R.; Brooks, C. Measuring Follow-up Time in Routinely-Collected Health Datasets: Challenges and Solutions. PLoS ONE 2020, 15, e0228545. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Peteresen, I.; Sørensen, H.T.; von Elm, E.; Langan, S.M. The REporting of Studies Conducted Using Observational Routinely-Collected Health Data (RECORD) Statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef]
- Garland, A.; Olafson, K.; Ramsey, C.D.; Yogendran, M.; Fransoo, R. A Population-Based Observational Study of Intensive Care Unit-Related Outcomes with Emphasis on Post-Hospital Outcomes. Ann. Am. Thorac. Soc. 2015, 12, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Chesley, C.F.; Harhay, M.O.; Small, D.S.; Hanish, A.; Prescott, H.C.; Mikkelsen, M.E. Hospital Readmission and Post-Acute Care Use After Intensive Care Unit Admissions: New ICU Quality Metrics? J. Intensive Care Med. 2022, 37, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Hirshberg, E.L.; Wilson, E.L.; Stanfield, V.; Kuttler, K.G.; Majercik, S.; Beesley, S.J.; Orme, J.; Hopkins, R.O.; Brown, S.M. Impact of Critical Illness on Resource Utilization: A Comparison of Use in the Year Before and After ICU Admission. Crit. Care Med. 2019, 47, 1497–1504. [Google Scholar] [CrossRef] [PubMed]
- van Beusekom, I.; Bakhshi-Raiez, F.; de Keizer, N.F.; van der Schaaf, M.; Termorshuizen, F.; Dongelmans, D.A. Dutch ICU Survivors Have More Consultations with General Practitioners before and after ICU Admission Compared to a Matched Control Group from the General Population. PLoS ONE 2019, 14, e0217225. [Google Scholar] [CrossRef] [PubMed]
- Jeitziner, M.M.; Zwakhalen, S.M.G.; Hantikainen, V.; Hamers, J.P.H. Healthcare Resource Utilisation by Critically Ill Older Patients Following an Intensive Care Unit Stay. J. Clin. Nurs. 2015, 24, 1347–1356. [Google Scholar] [CrossRef]
- Guillon, A.; Hermetet, C.; Barker, K.A.; Jouan, Y.; Gaborit, C.; Ehrmann, S.; le Manach, Y.; Dequin, P.F.; Grammatico-Guillon, L. Long-Term Survival of Elderly Patients after Intensive Care Unit Admission for Acute Respiratory Infection: A Population-Based, Propensity Score-Matched Cohort Study. Crit. Care 2020, 24, 384. [Google Scholar] [CrossRef]
- Keizer, E.; Smits, M.; Peters, Y.; Huibers, L.; Giesen, P.; Wensing, M. Contacts with Out-of-Hours Primary Care for Nonurgent Problems: Patients’ Beliefs or Deficiencies in Healthcare? Knowledge, Attitudes, Behaviors, Education, and Communication. BMC Med. Res. Methodol. 2015, 15, 157. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.; Hunt, M.; Muscedere, J.; Maslove, D.M.; Lee, J. Using Consumer-Grade Physical Activity Trackers to Measure Frailty Transitions in Older Critical Care Survivors: Exploratory Observational Study. JMIR Aging 2021, 4, e19859. [Google Scholar] [CrossRef]
- Shankar-Hari, M.; Rubenfeld, G.D.; Ferrando-Vivas, P.; Harrison, D.A.; Rowan, K. Development, Validation, and Clinical Utility Assessment of a Prognostic Score for 1-Year Unplanned Rehospitalization or Death of Adult Sepsis Survivors. JAMA Netw. Open 2020, 3, e2013580. [Google Scholar] [CrossRef]
- Welch, C.A.; Harrison, D.A.; Hutchings, A.; Rowan, K. The Association between Deprivation and Hospital Mortality for Admissions to Critical Care Units in England. J. Crit. Care 2010, 25, 382–390. [Google Scholar] [CrossRef]
- Ranzani, O.T.; Zampieri, F.G.; Besen, B.A.M.P.; Azevedo, L.C.P.; Park, M. One-Year Survival and Resource Use after Critical Illness: Impact of Organ Failure and Residual Organ Dysfunction in a Cohort Study in Brazil. Crit. Care 2015, 19, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pugh, R.J.; Bailey, R.; Szakmany, T.; al Sallakh, M.; Hollinghurst, J.; Akbari, A.; Griffiths, R.; Battle, C.; Thorpe, C.; Subbe, C.P.; et al. Long-Term Trends in Critical Care Admissions in Wales. Anaesthesia 2021, 76, 1316–1325. [Google Scholar] [CrossRef] [PubMed]
- Szakmany, T.; Hollinghurst, J.; Pugh, R.; Akbari, A.; Griffiths, R.; Bailey, R.; Lyons, R.A. Frailty Assessed by Administrative Tools and Mortality in Patients with Pneumonia Admitted to the Hospital and ICU in Wales. Sci. Rep. 2021, 11, 13407. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Overall | |
|---|---|
| (n = 55,151) | |
| Sex | |
| Male | 29,604 (53.7%) |
| Female | 25,547 (46.3%) |
| Age | |
| Median (IQR) | 66.0 (24.3) |
| Mean (SD) | 62.4 (17.9) |
| Groups | |
| 16–49 years | 12,624 (22.9%) |
| 50–59 years | 7752 (14.1%) |
| 60–69 years | 12,716 (23.1%) |
| 70–79 years | 13,651 (24.8%) |
| 80+ years | 8408 (15.2%) |
| 2011 Welsh Index of Multiple Deprivation, quintiles | |
| Most deprived | 12,964 (23.5%) |
| Next most deprived | 12,224 (22.2%) |
| Middle deprivation | 11,758 (21.3%) |
| Next least deprived | 9549 (17.3%) |
| Least deprived | 8656 (15.7%) |
| Charlson Comorbidity Index (modified) | |
| Median (IQR) | 7.00 (14.0) |
| Mean (SD) | 9.18 (9.70) |
| Categories | |
| Low (<1) | 16,496 (29.9%) |
| Medium (1 to <10) | 17,793 (32.3%) |
| High (≥10) | 20,862 (37.8%) |
| Follow-up in SAIL | |
| 1 year before critical care | |
| Median (IQR) | 365 (0) |
| Mean (SD) | 365 (0) |
| 1 year after critical care | |
| Median (IQR) | 365 (0) |
| Mean (SD) | 311 (116) |
| Follow-up in the GP data | |
| 1 year before critical care | |
| Median (IQR) | 365 (0) |
| Mean (SD) | 362 (27.9) |
| Missing | 13,534 (24.5%) |
| 1 year after critical care | |
| Median (IQR) | 365 (0) |
| Mean (SD) | 328 (93.5) |
| Missing | 16,607 (30.1%) |
| GP events | |
| 1 year before critical care | |
| Median (IQR) | 32.0 (28.0) |
| Mean (SD) | 35.6 (23.7) |
| Missing | 13,534 (24.5%) |
| 1 year after critical care | |
| Median (IQR) | 37.0 (34.0) |
| Mean (SD) | 39.5 (26.5) |
| Missing | 16,607 (30.1%) |
| Outpatient attendances | |
| 1 year before critical care | |
| Median (IQR) | 3.00 (6.00) |
| Mean (SD) | 5.17 (6.13) |
| 1 year after critical care | |
| Median (IQR) | 4.00 (7.56) |
| Mean (SD) | 6.11 (7.06) |
| ED attendances | |
| 1 year before critical care | |
| Median (IQR) | 1.00 (2.00) |
| Mean (SD) | 1.21 (1.78) |
| 1 year after critical care | |
| Median (IQR) | 0.00 (1.00) |
| Mean (SD) | 0.85 (1.79) |
| Length of hospital stay | |
| 1 year before critical care | |
| Median (IQR) | 2.00 (10.0) |
| Mean (SD) | 9.67 (22.1) |
| 1 year after critical care | |
| Median (IQR) | 10.0 (26.0) |
| Mean (SD) | 26.2 (44.0) |
| GP Consultations | Outpatient Attendances | ED Attendances | Length of Hospital Stay | |||||
|---|---|---|---|---|---|---|---|---|
| IRR (95% CI) | p Value | IRR (95% CI) | p Value | IRR (95% CI) | p Value | IRR (95% CI) | p Value | |
| Most deprived | 0.983 (0.967, 0.999) | 0.043 | 0.967 (0.944, 0.991) | 0.007 | 1.237 (1.158, 1.320) | <0.001 | 1.128 (1.085, 1.171) | <0.001 |
| Next most deprived | 0.997 (0.981, 1.014) | 0.759 | 0.982 (0.959, 1.006) | 0.149 | 1.157 (1.083, 1.236) | 0.000 | 1.061 (1.021, 1.102) | 0.003 |
| Middle deprivation | 1.018 (1.001, 1.035) | 0.040 | 0.946 (0.923, 0.969) | <0.001 | 1.104 (1.033, 1.179) | 0.004 | 1.049 (1.009, 1.091) | 0.015 |
| Next least deprived | 1.014 (0.996, 1.032) | 0.127 | 0.944 (0.920, 0.968) | <0.001 | 1.107 (1.033, 1.187) | 0.004 | 0.995 (0.956, 1.037) | 0.827 |
| CCI: medium | 1.133 (1.118, 1.148) | <0.001 | 1.224 (1.200, 1.248) | <0.001 | 1.200 (1.141, 1.263) | <0.001 | 1.003 (0.973, 1.035) | 0.825 |
| CCI: high | 1.221 (1.204, 1.238) | <0.001 | 1.474 (1.445, 1.504) | <0.001 | 1.429 (1.357, 1.505) | <0.001 | 1.622 (1.572, 1.674) | <0.001 |
| Age 50–59 | 1.141 (1.122, 1.161) | <0.001 | 1.123 (1.095, 1.152) | <0.001 | 0.798 (0.748, 0.851) | <0.001 | 1.470 (1.413, 1.531) | <0.001 |
| Age 60–69 | 1.150 (1.132, 1.168) | <0.001 | 1.127 (1.102, 1.153) | <0.001 | 0.783 (0.738, 0.830) | <0.001 | 1.655 (1.596, 1.716) | <0.001 |
| Age 70–79 | 1.134 (1.116, 1.152) | <0.001 | 1.029 (1.006, 1.053) | 0.013 | 0.768 (0.723, 0.815) | <0.001 | 2.059 (1.986, 2.135) | <0.001 |
| Age 80+ | 1.114 (1.093, 1.135) | <0.001 | 0.853 (0.831, 0.877) | <0.001 | 0.831 (0.777, 0.890) | <0.001 | 2.963 (2.844, 3.086) | <0.001 |
| Female | 1.005 (0.995, 1.015) | 0.340 | 0.979 (0.964, 0.994) | 0.005 | 0.964 (0.928, 1.002) | 0.065 | 0.972 (0.949, 0.995) | 0.017 |
| Event count in the previous year | 1.013 (1.013, 1.014) | <0.001 | 1.058 (1.056, 1.059) | <0.001 | 1.258 (1.246, 1.269) | <0.001 | 1.013 (1.013, 1.014) | <0.001 |
| Intercept | 0.062 (0.060, 0.063) | <0.001 | 0.012 (0.011, 0.012) | <0.001 | 0.002 (0.002, 0.002) | <0.001 | 0.060 (0.057, 0.062) | <0.001 |
| GP Consultations | Outpatient Attendances | ED Attendances | Length of Hospital Stay | |||||
|---|---|---|---|---|---|---|---|---|
| Change (95% CI) | p Value | Change (95% CI) | p Value | Change (95% CI) | p Value | Change (95% CI) | p Value | |
| Most deprived | −0.47 (−1.49, 0.54) | 0.360 | −0.08 (−0.35, 0.20) | 0.580 | 0.24 (0.12, 0.36) | <0.001 | 6.94 (4.35, 9.53) | <0.001 |
| Next most deprived | 0.25 (−0.78, 1.28) | 0.633 | 0.03 (−0.25, 0.30) | 0.840 | 0.18 (0.06, 0.31) | 0.003 | 3.61 (1.01, 6.22) | 0.007 |
| Middle deprivation | 1.42 (0.38, 2.46) | 0.007 | −0.22 (−0.50, 0.05) | 0.111 | 0.10 (−0.02, 0.22) | 0.099 | 3.45 (0.83, 6.07) | 0.010 |
| Next least deprived | 0.69 (−0.42, 1.80) | 0.222 | −0.30 (−0.58, −0.01) | 0.045 | 0.18 (0.05, 0.30) | 0.007 | −0.18 (−2.92, 2.57) | 0.900 |
| CCI: medium | 3.95 (3.12, 4.77) | <0.001 | 1.10 (0.88, 1.32) | <0.001 | 0.20 (0.11, 0.30) | <0.001 | −0.76 (−2.83, 1.31) | 0.473 |
| CCI: high | 8.83 (7.97, 9.69) | <0.001 | 2.49 (2.27, 2.72) | <0.001 | 0.29 (0.19, 0.39) | <0.001 | 27.62 (25.50, 29.74) | <0.001 |
| Age 50–59 | 4.03 (2.96, 5.09) | <0.001 | 0.68 (0.40, 0.97) | <0.001 | −0.21 (−0.34, −0.09) | <0.001 | 12.49 (9.77, 15.21) | <0.001 |
| Age 60–69 | 3.64 (2.67, 4.61) | <0.001 | 0.64 (0.38, 0.90) | <0.001 | −0.21 (−0.33, −0.10) | <0.001 | 17.96 (15.51, 20.40) | <0.001 |
| Age 70–79 | 3.23 (2.25, 4.21) | <0.001 | −0.28 (−0.54, −0.02) | 0.032 | −0.22 (−0.34, −0.11) | <0.001 | 31.12 (28.68, 33.57) | <0.001 |
| Age 80+ | 2.98 (1.85, 4.12) | <0.001 | −1.58 (−1.87, −1.29) | <0.001 | −0.24 (−0.37, −0.12) | <0.001 | 59.13 (56.37, 61.89) | <0.001 |
| Female | −0.37 (−1.01, 0.26) | 0.252 | −0.26 (−0.43, −0.10) | 0.002 | −0.05 (−0.12, 0.03) | 0.198 | 0.13 (−1.46, 1.72) | 0.874 |
| Event count in the previous year | −0.31 (−0.32, −0.30) | <0.001 | −0.45 (−0.47, −0.44) | <0.001 | −0.52 (−0.54, −0.50) | <0.001 | −0.13 (−0.16, −0.09) | <0.001 |
| Intercept | 16.65 (15.55, 17.75) | <0.001 | 3.74 (3.45, 4.04) | <0.001 | 0.48 (0.35, 0.62) | <0.001 | 18.92 (16.18, 21.66) | <0.001 |
| Critical Care Sub-Cohort | Non-Critical-Care Hospital Population | Overall | |
|---|---|---|---|
| (n = 5204) | (n = 200,000) | (n = 205,204) | |
| Sex | |||
| Male | 2837 (54.5%) | 85,109 (42.6%) | 87,946 (42.9%) |
| Female | 2367 (45.5%) | 114,891 (57.4%) | 117,258 (57.1%) |
| Age | |||
| Median (IQR) | 66.0 (23.7) | 61.5 (32.8) | 61.7 (32.5) |
| Mean (SD) | 62.5 (17.7) | 57.9 (20.4) | 58.0 (20.4) |
| Groups | |||
| <50 | 1156 (22.2%) | 67,884 (33.9%) | 69,040 (33.6%) |
| 50–59 | 797 (15.3%) | 27,417 (13.7%) | 28,214 (13.7%) |
| 60–69 | 1227 (23.6%) | 37,888 (18.9%) | 39,115 (19.1%) |
| 70–79 | 1239 (23.8%) | 38,249 (19.1%) | 39,488 (19.2%) |
| 80+ | 785 (15.1%) | 28,562 (14.3%) | 29,347 (14.3%) |
| 2011 Welsh Index of Multiple Deprivation, quintiles | |||
| Most deprived | 1164 (22.4%) | 41,722 (20.9%) | 42,886 (20.9%) |
| Next most deprived | 1162 (22.3%) | 42,030 (21.0%) | 43,192 (21.0%) |
| Middle deprivation | 1161 (22.3%) | 40,819 (20.4%) | 41,980 (20.5%) |
| Next least deprived | 975 (18.7%) | 38,332 (19.2%) | 39,307 (19.2%) |
| Least deprived | 742 (14.3%) | 37,097 (18.5%) | 37,839 (18.4%) |
| Charlson Comorbidity Index (modified) | |||
| Median (IQR) | 7.00 (14.0) | 2.00 (9.00) | 3.00 (10.0) |
| Mean (SD) | 9.07 (9.42) | 6.35 (8.99) | 6.42 (9.01) |
| Categories | |||
| Low (<1) | 1505 (28.9%) | 99,752 (49.9%) | 101,257 (49.3%) |
| Medium (1 to <10) | 1740 (33.4%) | 50,630 (25.3%) | 52,370 (25.5%) |
| High (≥10) | 1959 (37.6%) | 49,618 (24.8%) | 51,577 (25.1%) |
| Follow-up in SAIL | |||
| 1 year before critical care | |||
| Median (IQR) | 365 (0) | 365 (0) | 365 (0) |
| Mean (SD) | 365 (0) | 361 (31.5) | 361 (31.1) |
| 1 year after critical care | |||
| Median (IQR) | 365 (0) | 365 (0) | 365 (0) |
| Mean (SD) | 330 (90.9) | 339 (78.7) | 338 (79.1) |
| Follow-up in the GP data | |||
| 1 year before critical care | |||
| Median (IQR) | 365 (0) | 365 (0) | 365 (0) |
| Mean (SD) | 361 (30.8) | 358 (40.3) | 358 (40.1) |
| Missing | 1275 (24.5%) | 47,604 (23.8%) | 48,879 (23.8%) |
| 1 year after critical care | |||
| Median (IQR) | 365 (0) | 365 (0) | 365 (0) |
| Mean (SD) | 327 (95.2) | 335 (83.2) | 335 (83.6) |
| Missing | 1276 (24.5%) | 47,547 (23.8%) | 48,823 (23.8%) |
| GP consultations | |||
| 1 year before critical care | |||
| Median (IQR) | 26.0 (43.0) | 23.0 (36.0) | 24.0 (36.0) |
| Mean (SD) | 28.0 (25.8) | 26.9 (24.9) | 27.0 (24.9) |
| 1 year after critical care | |||
| Median (IQR) | 31.0 (52.0) | 22.0 (39.0) | 22.0 (40.0) |
| Mean (SD) | 32.6 (29.4) | 26.0 (25.9) | 26.2 (26.0) |
| ED attendances | |||
| 1 year before critical care | |||
| Median (IQR) | 1.00 (2.00) | 0 (1.00) | 0 (1.00) |
| Mean (SD) | 1.20 (1.77) | 0.861 (1.81) | 0.870 (1.81) |
| 1 year after critical care | |||
| Median (IQR) | 0 (1.00) | 0 (1.00) | 0 (1.00) |
| Mean (SD) | 0.960 (1.67) | 0.756 (1.92) | 0.761 (1.91) |
| Outpatient attendances | |||
| 1 year before critical care | |||
| Median (IQR) | 3.00 (6.00) | 4.00 (7.00) | 4.00 (7.00) |
| Mean (SD) | 5.14 (6.08) | 5.76 (6.60) | 5.74 (6.59) |
| 1 year after critical care | |||
| Median (IQR) | 5.00 (7.00) | 4.00 (7.00) | 4.00 (7.00) |
| Mean (SD) | 6.74 (6.92) | 5.65 (6.89) | 5.68 (6.89) |
| Length of hospital stay, days | |||
| 1 year before critical care | |||
| Median (IQR) | 1.00 (7.00) | 2.00 (12.0) | 2.00 (12.0) |
| Mean (SD) | 7.83 (17.8) | 12.9 (29.6) | 12.8 (29.3) |
| 1 year after critical care | |||
| Median (IQR) | 12.0 (29.0) | 3.00 (14.0) | 3.00 (15.0) |
| Mean (SD) | 29.0 (44.9) | 15.0 (32.7) | 15.3 (33.1) |
| GP Consultations | Outpatient Attendances | ED Attendances | Length of Hospital Stay | |||||
|---|---|---|---|---|---|---|---|---|
| IRR (95% CI) | p Value | IRR (95% CI) | p Value | IRR (95% CI) | p Value | IRR (95% CI) | p Value | |
| Critical care | 1.07 (1.06, 1.08) | 0.001 | 1.09 (1.07, 1.11) | <0.001 | 1.12 (1.07, 1.16) | <0.001 | 1.68 (1.63, 1.74) | <0.001 |
| CCI: medium | 1.21 (1.20, 1.22) | <0.001 | 1.41 (1.40, 1.43) | <0.001 | 1.35 (1.32, 1.38) | <0.001 | 1.70 (1.66, 1.74) | <0.001 |
| CCI: high | 1.21 (1.21, 1.22) | <0.001 | 1.56 (1.54, 1.58) | <0.001 | 1.75 (1.70, 1.79) | <0.001 | 2.65 (2.59, 2.72) | <0.001 |
| Most deprived | 1.10 (1.09, 1.11) | <0.001 | 1.00 (0.98, 1.02) | 0.870 | 1.47 (1.42, 1.52) | <0.001 | 1.29 (1.24, 1.34) | <0.001 |
| Next most deprived | 1.08 (1.07, 1.10) | <0.001 | 0.99 (0.97, 1.01) | 0.422 | 1.35 (1.31, 1.40) | <0.001 | 1.19 (1.14, 1.23) | <0.001 |
| Middle deprivation | 1.07 (1.06, 1.08) | <0.001 | 0.98 (0.97, 1.00) | 0.066 | 1.27 (1.23, 1.31) | <0.001 | 1.12 (1.08, 1.17) | <0.001 |
| Next least deprived | 1.06 (1.05, 1.07) | <0.001 | 0.99 (0.97, 1.01) | 0.372 | 1.09 (1.05, 1.12) | <0.001 | 1.04 (1.00, 1.08) | <0.060 |
| Age 50–59 | 1.39 (1.37, 1.40) | <0.001 | 1.36 (1.33, 1.38) | <0.001 | 0.86 (0.83, 0.89) | <0.001 | 1.13 (1.09, 1.18) | <0.001 |
| Age 60–69 | 1.58 (1.57, 1.60) | <0.001 | 1.50 (1.48, 1.53) | <0.001 | 0.84 (0.81, 0.86) | <0.001 | 1.55 (1.49, 1.61) | <0.001 |
| Age 70–79 | 1.74 (1.72, 1.75) | <0.001 | 1.55 (1.52, 1.57) | <0.001 | 1.00 (0.97, 1.03) | 0.862 | 2.16 (2.08, 2.24) | <0.001 |
| Age 80+ | 1.87 (1.85, 1.89) | <0.001 | 1.24 (1.21, 1.26) | <0.001 | 1.52 (1.47, 1.57) | <0.001 | 3.87 (3.72, 4.03) | <0.001 |
| Female | 1.04 (1.03, 1.04) | <0.001 | 0.95 (0.94, 0.96) | <0.001 | 0.90 (0.88, 0.92) | <0.001 | 1.09 (1.06, 1.12) | <0.001 |
| Event count in the previous year | 1.01 (1.01, 1.01) | <0.001 | 1.01 (1.01, 1.01) | <0.001 | 1.08 (1.08, 1.08) | <0.001 | 0.99 (0.99, 0.99) | <0.001 |
| Intercept | 0.04 (0.03, 0.04) | <0.001 | 0.01 (0.01, 0.01) | <0.001 | 0.00 (0.00, 0.00) | <0.001 | 0.00 (0.00, 0.00) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsallakh, M.; Tan, L.; Pugh, R.; Akbari, A.; Bailey, R.; Griffiths, R.; Lyons, R.A.; Szakmany, T. Patterns of Healthcare Resource Utilisation of Critical Care Survivors between 2006 and 2017 in Wales: A Population-Based Study. J. Clin. Med. 2023, 12, 872. https://doi.org/10.3390/jcm12030872
Alsallakh M, Tan L, Pugh R, Akbari A, Bailey R, Griffiths R, Lyons RA, Szakmany T. Patterns of Healthcare Resource Utilisation of Critical Care Survivors between 2006 and 2017 in Wales: A Population-Based Study. Journal of Clinical Medicine. 2023; 12(3):872. https://doi.org/10.3390/jcm12030872
Chicago/Turabian StyleAlsallakh, Mohammad, Laura Tan, Richard Pugh, Ashley Akbari, Rowena Bailey, Rowena Griffiths, Ronan A. Lyons, and Tamas Szakmany. 2023. "Patterns of Healthcare Resource Utilisation of Critical Care Survivors between 2006 and 2017 in Wales: A Population-Based Study" Journal of Clinical Medicine 12, no. 3: 872. https://doi.org/10.3390/jcm12030872